

About Authors:
Dhakar Mukesh*, M. Jeevan, Kumar Neeraj, Dashora Ashok
Geetanjali Institute of Pharmacy,
(Department of Pharmaceutical Chemistry.)
AirPort Road, Dabok, Udaipur (Rajasthan)- 313022
*dhakarmukesh03@yahoo.com
Abstract:
Antioxidants are essential and important for plants and animals’ sustenance. They are substances that protect cells from the damage caused by unstable molecules known as free radicals. Cancer develops when cells multiply in the presence of oxidation and other damage. Certain "antioxidant" substances, such as vitamin C, are able to exploit the differences between cancer and healthy cells; they kill cancer cells while helping healthy cells. Antioxidants are substances that may protect cells from the damage caused by unstable molecules known as free radicals. Free radical damage may lead to cancer. Antioxidants interact with and stabilize free radicals and may prevent some of the damage free radicals Examples of antioxidants include Quercetin Curcumin Beta-carotene, Lycopene, Vitamins C, E, and A, and other substances. Epidemiological studies have consistently shown that regular consumption of fruits and vegetables is strongly associated with reduced risk of developing chronic diseases, such as cancer and cardiovascular disease.[1]
Reference Id: PHARMATUTOR-ART-1968
Introduction:
Antioxidants neutralize free radicals as the natural by-product of normal cell processes.
Free radical formation can leads due to the Exposure of various environmental factors, including tobacco smoke and radiation and etc. The most common form of free radicals in Humans is oxygen. When an oxygen molecule becomes electrically charged causing damage to the DNA and other Cell such damage may be irreversible and may be causes many disorders like as Cancer. Antioxidants are neutralize the electrical charge and prevent the transportation of electrons from other molecules to free radicals.
DNA is a major target of free radical damage. The types of damages induced are many and include strand breaks (single or double strand breaks) damage yielding products such as 8-hydroxyguanosine, thymine glycol or a basic sites. These damages can result in mutations that are heritable change in the DNA that can yield cancer. The involvement of free radicals with tumor suppressor genes and proto-oncogenes suggest their role in the development of different human cancer.[2]
produced in the body (endogenous) and others obtained from the diet (exogenous Humans have evolved with antioxidant systems for protection against free radicals and ROS. These systems include some antioxidants).[19]
Many clinical trials published and reached differing conclusions about the effect of antioxidants on cancer.
1. The first large randomized trial on antioxidants and cancer risk was the Chinese Cancer Prevention Study, published in 1993. This trial investigated the effect of a combination of beta-carotene, vitamin E, and selenium on cancer in healthy Chinese men and women at high risk for gastric cancer. The study showed a combination of beta-carotene, vitamin E, and selenium significantly reduced incidence of both gastric cancer and cancer overall. [3]
2. A 1994 cancer prevention study entitled the Alpha-Tocopherol (vitamin E)/ Beta-Carotene Cancer Prevention Study (ATBC) demonstrated that lung cancer rates of Finnish male smokers increased significantly with beta-carotene and were not affected by vitamin E. [4]
Cancer development can be described by three stages: initiation, promotion and progression, and ROS can act in all these stages of carcinogenesis [5] . It is also well established that free radicals are known to react with all components of DNA, thus damaging its bases and the deoxyribose backbone [6] causing mutations in crucial genes, which ultimately may lead to cancer. [7]
A high level of oxidative stress can induce apoptosis or even necrosis; however, a low level of oxidative stress can stimulate cell division and thus promote tumor growth. [8] ROS probably enhance the final irreversible stage of carcinogenesis, which is characterized by accumulation of additional genetic damage, leading to the transition of the cell from benign to malignant.
Three large-scale clinical trials continue to investigate the effect of antioxidants on cancer
1. The Women’s Health Study (WHS) is currently evaluating the effect of vitamin E in the primary prevention of cancer among U.S. female health professionals age 45 and older. The WHS is expected to conclude in August 2004
2. The Selenium and Vitamin E Cancer Prevention Trial (SELECT) is taking place in the United States, Puerto Rico, and Canada. SELECT is trying to find out if taking selenium and/or vitamin E supplements can prevent prostate cancer in men age 50 or older. The SELECT trial is expected to stop recruiting patients in May 2006.
3. The Physicians' Health Study II (PHS II) is a follow up to the earlier clinical trial by the same name. The study is investigating the effects of vitamin E, C, and multivitamins on prostate cancer and total cancer incidence. The PHS II is expected to conclude in August 2007.[9_11]
Last stages cancer can’t treated with antioxidants suppliments. So ant oxidative nutritional supplements as cancer preventatives is not actual therapies [14].The great Caltech chemist, Linus Pauling, who near the end of his illustrious career wrote a book with Ewan Cameron in 1979, Cancer and Vitamin C, about vitamin C's great potential as an anti-cancer agent.[12]. But At the time of his death from prostate cancer in 1994, at the age of 93, Linus was taking 12 g of vitamin C every day. late-stage cancer'. vast number of nutritional intervention trials using the antioxidants β-carotene, vitamin A, vitamin C, vitamin E and selenium have shown no obvious effectiveness in preventing gastrointestinal cancer.[13].
The cytotoxic action (side/adverse effect of anti cancer agents) of many anticancer drug including like as 5-fluorouracil, vincristine, doxorubicin, cisplatin and were found to be increased with co administration or in presence of vitamin E and the cytotoxic effect of Antineoplastics agents Bleomycin, Paclitaxel and darcarbazine were found to be increased with co administration or in presence of vitamin C during in vitro studies through inhibition of the effects of lipid peroxidise on cell growth. [15].
Molecular Studies of Natural Antioxidants:
Different types of natural antioxidants are present in fruit and vegetables they have synergistic interactions that are important due to their activity and regenerative potential. For example,ascorbate can regenerate into α-tocopherol. [16] Interactions is known as the “antioxidant network”.
Tumor necrosis factor-alpha (TNF-α) is a cytokine that, under normal conditions, induces inflammation, tumor inhibition, and apoptotic cell death. However, when the former undergoes deregulation, it acts as a breast tumor promoter, enhancing the proliferation of chemically induced mammary tumors. [17].
Phenolic antioxidants can block the increase of TNF- α at the transcriptional level in the nucleus, which suggests the molecular mechanism of phenolic antioxidants through control of cytokine induction. [18].
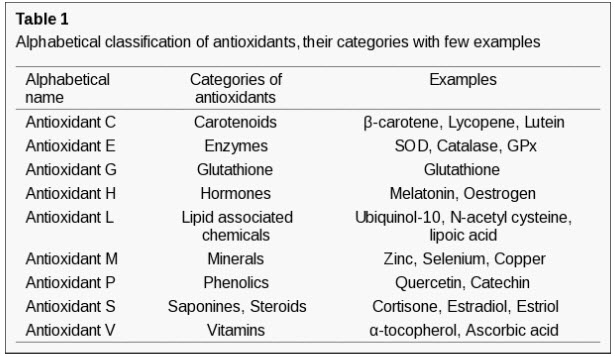
Nomenclature and Classification of Antioxidants:
Table 1 lists categories in which various antioxidants have been characterized.
ANTIOXIDANT AGENTS:
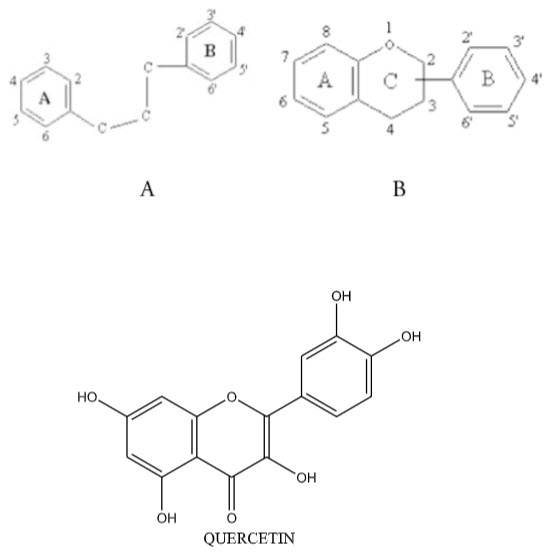
1.) QUERCETIN:
Quercetin (3,3’,4’,5,7-pentahydroxyflavone)is one of the most frequently studied bioflavonoid. Flavonoids are polyphenolic compounds possessing 15 carbon atoms, two benzene rings joined by a linear three carbon atom chain (structure A). The chemical structure of flavonoids are based on a C15 skeleton with a chromane ring bearing a second aromatic ring B in position 2, 3 or 4 (structure B). Quercetin have multiple pharmacological and medicinal action and uses as anti-inflammatory, anti-allergic, antiviral, antithrombotic, anti-mutagenic and antineoplasti agents. [20]
A number of its actions make it a potential anti-cancer agent, including cell cycle regulation, interaction with type II estrogen binding sites, and tyrosine kinase inhibition. [21].
Its reputation as an antioxidant stems from the reactivity of phenolic compounds with free radical species to form phenoxy radicals which are considerably less reactive
Properties, Occurrence and Production of Quercetin:
Quercetin is a yellow, crystalline solid with a bitter taste, which is insoluble in water, slightly soluble in alcohol, and soluble in glacial acetic acid and aqueous alkaline solutions.[22_23]. Quercetin is usually obtained from the hydrolysis of rutin (quercetin-3- rutinoside), a naturally occurring flavonoid glycoside. [24] although it can also be synthesized.[25] Quercetin glycosides are relatively poorly absorbed by the small intestine. Micro flora of the lower bowel hydrolyze the flavonide-glycoside to quercetin and the sugar, and quercetin is then absorbed into the enterohepatic system [26-28]. A 100 mg single dose was found to create a serum concentration of 0.8 microM quercetin, The serum quercetin concentrations required for anti-cancer activity (upwards of 10 microM,[29]. Quercetin interfere by reacting with the radicals formed in the process of lipid peroxidation[30]
Table 2. Quercetin Content in Selected Foods:
|
Food Source |
Quercetin Content (mg/100g) |
|
Apple with skin |
4.42 |
|
Raw Onions |
13.27 |
|
Black Tea Leaves, dry |
204.66 |
Green Tea Leaves, dry |
255.55 |
Quercetin have a ability to scavenge free radicals and bind transition metal ions. These properties of quercetin allow it to inhibit lipid peroxidation [31-32].
ANTI-CANCER EFFECTS OF QUERCETIN:
Oxidative DNA damage is a known risk factor of cancer. Antioxidants, such as quercetin, are thought to play an important role in protecting cells from oxidative stress induced by reactive oxygen species(ROS). ROS and RNS (reactive nitrogen species) play a vital role in development of Cancer in Human. ROS is collective term of various oxidizing agents.[33]
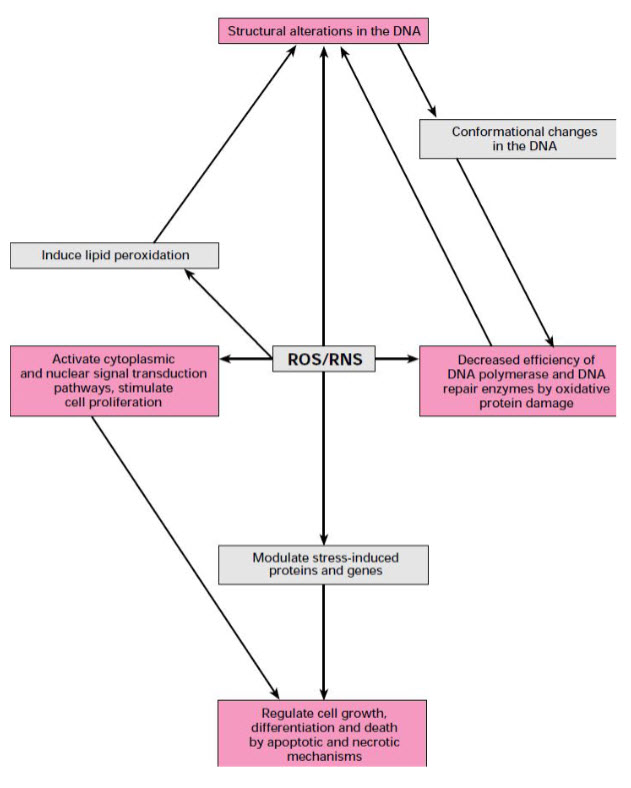
Fig. : Role of ROS/RNS in cancer development [33]
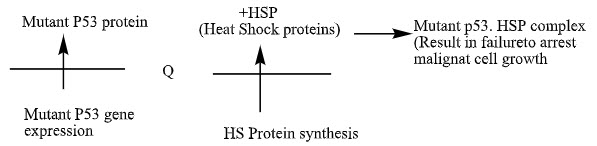
MOLECULAR MECHANISM OF ACTION OF QUERCETIN:
1.) Down Regulation of Mutant P53 Protein:
Quercetin (248 microM) was found to down regulate expression of mutant p53 protein to nearly undetectable levels in human breast cancer cell lines. Lower concentrations gave less reduction [34-37].
1.) G1 phase arrest:
The G1 checkpoint controlled by the p53 gene is a major site for the control of cellular proliferation. Quercetin has been found to arrest human leukemic T-cells in the late G1 phaseof the cell cycle.[38]
This G1 arrest was also seen in gastric cancer cells treated with Quercetin.
2.) Tyrosine Kinase Inhibition:
Tyrosine kinases are a family of proteins located in or near the cell membrane and involved in transduction of growth factor signal to nucleus. lymphocyte tyrosine kinase can be inhibited by the Quercetin on I.V. administration at a one hour time.[39-41].
3.) Estrogen receptor binding capacity:
Quercetin has been shown to induce ER II expression in both type I estrogen receptor positive (ER+) and type I estrogen receptor negative (ER-) human breast cancer cells. induction of ER II allows for greater growth inhibition of ER- cells with quercetin treatment. In cultured human melanoma cells, quercetin was found to bind ER II sites with an affinity similar to tamoxifen and diethylstilbestrol. ER II sites are found in normal tissue and on many different human tumor types, including breast, ovarian, colorectal, meningeal, leukemic, and melanoma.[42-44].

Use of Quercetin with Standard Oncologic Therapeutics:
1.) topical and oral administration of quercetin to reduce skin damage during radiotherapy in patients with head and neck cancers[45]
2.) Quercetin has been shown to increase the therapeutic efficacy of cisplatin both in vivo and in vitro.[46]
3.) An absence of potentiation of the effect of adriamycin or etoposide due to quercetin administration was noted.[47]
4.) Quercetin (10-100 microM) has also been shown in vitro to protect normal renal tubular cells from cisplatin toxicity.[48]
5.) Quercetin has also been shown in vitro to increase the cytotoxic effect of cyclophosphamide.[49]
6.) Decrease the resistance to gemcitabine and topotecan. [50]
2.) SELENIUM:
Selenium is a chemical element with symbol Se and atomic number 34. Selenium is found in cereals, meat, poultry, seafood, and eggs. Cereals may provide about 50% of dietary selenium, however data on the selenium content of Australian foods is limited. The selenium content of plant foods varies with the selenium content of the soil. Selenium acts as an antioxidant and helps protect the body against the damaging effects of free radicals. Selenium is essential for the activity of glutathione peroxidase, an enzyme that protects against reactive oxygen species and subsequent cell membrane damage.[51]
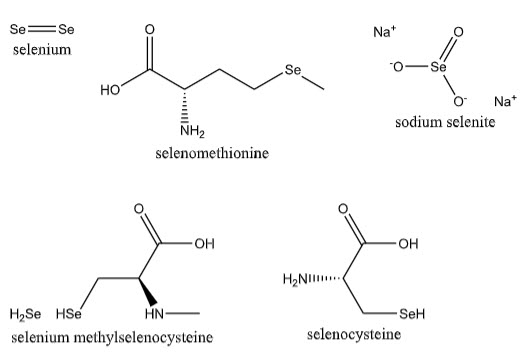
Selenium exists in many forms. The most well studied include selenomethionine (SeMet), sodium selenite, selenium methylselenocysteine (SeMeSC), 1,4,-phenylenebis (methylene) selenocyanate (p-XSC), and methylseleninic acid (MSA).[52]
Selenium is a component of the antioxidant.the average daily dietary selenium (Se) intake in the United States is consistently above the adult RDA of 55 μg Se/day, supranutritional supplements of 200 μg Se/day have been shown to provide chemopreventive benefits against several cancers, particularly prostate cancer. selenium compounds contents the greatest anticarcinogenic potency are likely to be sodium selenite with Se in the +4 oxidation state and methylseleninic acid. These compounds exert their cancer chemopreventive effects by directly oxidizing critical thiol-containing cellular substrates, and are more effective than the more frequently preferred (used) supplements of selenomethionine and Se–methylselenocysteine that lack oxidation capability. Selenate (+6 Se) the immediate precursor of selenite (+4 Se) can be metabolically reduced, and although less potent than the +4 Se compounds cited above, appears to be a more effective anticarcinogen than organic forms of dietary selenium.
It is a potent modulator of eukaryotic cell growth with strictly concentration-dependant effects. Lower concentrations are necessary for cell survival and growth, whereas higher concentrations inhibit growth and induce cell death.[53]
The protective effect of this mineral is especially associated with its presence in glutathione peroxidase and thioredoxin reductase, enzymes that protect the DNA and other cellular components against oxidative damage caused by ROS. Several studies have demonstrated reduced expression of these enzymes in various types of cancer, especially when associated with a low intake of selenium, which may exacerbate the damage.[54]
Selenium increased the activity of cisplatin in mice, and decreased its toxicity in humans.
In recent years, selenium has become controversial following results from the large Selenium and Vitamin E Cancer Prevention Trial (SELECT), which was prematurely terminated after demonstrating no effect on prostate cancer risk [55]
MECHANISM OF ACTION OF SELENIUM:
A number of mechanisms have been suggested to explain the anti-cancer effects of Se. Although there is fairly general acceptance that methyl selenol (CH3SeH) is involved in the anti-cancer effects of Se at supra-nutritional doses.
|
Anti-cancer processes or pathways |
Selected evidence for Se involvement |
Reference |
|
Seleno-enzyme mechanisms Reduction of DNA damage |
Se intake or status affects DNA damage in both human and animal studies |
[56-58] |
|
Induction of phase II conjugating enzymes: detoxify carcinogens and reduce DNA adduct formation |
Some selenocompounds e.g. methyl selenol (CH3SeH), can up regulate phase II conjugating enzymes such as glutathione-S-transferase, increasing detoxification of carcinogens |
[59] |
|
Increase in tumour suppressor protein p53: inhibits proliferation, stimulates DNA repair and promotes apoptotic death by acting as a transcription factor |
SeMet can activate p53 through redox regulation of key p53 cysteine residues. Methyl seleninic acid (CH3SeO2H) and Na2SeO3 modulate p53 activity by Phosphorylation |
[60] |
Use of Selenium with Standard Oncologic Therapeutics:
1) selenium depletion reduces the lethal dose of radiation [61]
2) selenium decreased nephrotoxicity of cisplatin, while simultaneously increasing its anti tumor activity. [62].
3) seleniumcontaining antioxidant compound called Ebselen (2-phenyl-1,3-benzisoselenazol 3(2H)one) has a mild inhibitory effect on the anti-tumor effect of bleomycin. [63]
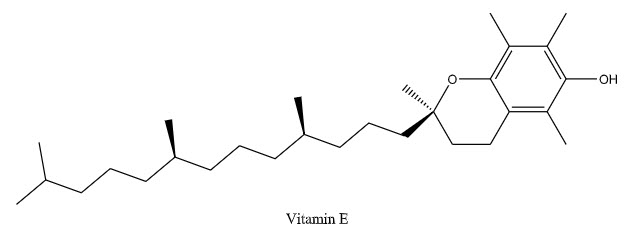
3. VITAMIN E:
Scientific/medical name(s)of vitamins E are alpha-tocopherol, tocopherols, tocotrienols,
Vitamin E is an essential fat-soluble nutrient that serves as an antioxidant and is also used in cell signaling, regulating gene expression and immune function. (Antioxidants block the action of free radicals, which are activated molecules that can damage cells.)
Vitamin E comprises a group of compounds possessing vitamin E activity. alpha- Tocopherol is the compound demonstrating the highest vitamin E activity, which is available both in its natural form as RRR-alpha-tocopherol isolated from plant sources, but more common as synthetically manufactured all-rac-alpha-tocopherol. Synthetic all-racalpha-tocopherol consists of a racemic mixture of all eight possible stereoisomers.[ 64]
The SELECT (Selenium and Vitamin E Cancer Prevention Trial) looked at the effect of vitamin E alone or in combination with selenium (an antioxidant mineral) on prostate cancer risk.
The ability of the vitamin E (RRR--tocopherol) derivatives -tocopheryl succinate (-TOS) and -tocopheryloxyacetic acid (-TEA) to suppress tumor growth.[65].
Vitamin E succinate (VES, alpha tocopherol succinate),has generated some interest as an adjunctive cancer therapy recently. VES demonstrated growth inhibition of human B-cell lymphoma. [66] With aim to evaluate the neuroprotective effect of antioxidant supplementation with vitamin E in patients treated with cisplatin chemotherapy. [67]
Research on human oral squamous carcinoma cells suggests the VES effect is biphasic; growth stimulatory at physiological concentrations, while pharmacological concentrations are inhibitory. [68]
Phase I clinical trials are being planned or are underway in patients with breast and prostate cancers.[69]Vitamin E and its derivatives are particularly attractive therapeutic agents due to their remarkable lack of toxicity in vivo. [70]
Vitamin E induces apoptosis in experimental tumor lines.Vitamin E with omega-3 fatty acids increased survival time in terminal cancer patients.Vitamin E in doses below 500 mg/kg (approximately 35,000 IU human dose) may increase the effect of radiotherapy in mice. Vitamin E increases the activity of 5- fluorouracil, doxorubicin, and cisplatin in vivo.No evidence exists that vitamin E reduces the effect of chemotherapy in vivo.[71]
Use of Vitamin E with Standard Oncologic Therapeutics:
1) Vitamin E(750mg/kg) have a greater anti- tumor activity with administration of 5- fluorouracil in mice bearing human colon cancer lines than either agent alone. Addition of vitamin E to either 5-fluorouracil or doxorubicin enhances the effect of these agents on human colon cancer cells. [72]
2) The tumor-bearing mice pretreated with vitamin E lived longer on average than those treated with doxorubicin alone the vitamin E blocked lipid peroxidation-mediated toxicity, while not impairing the anti-tumor property of doxorubicin. [73]
3) mice treated with 1 g/kg of vitamin E had an increased in the lethal radiation dose (LD50). [74]
4. Curcumin:
Curcumin is obtained from the Turmeric. Turmeric comes from the root of the Curcuma longa plant and has a tough brown skin and a deep orange flesh. Turmeric has long been used as a powerful anti-inflammatory in both the Chinese and Indian systems of medicine.
Curcumin have a strong antioxidant.
Antioxidant actions of Curcumin' enable it to protect the colon cells from free radicals that can damage cellular DNAâ?"a significant benefit particularly in the colon where cell turnover is quite rapid, occuring approximately every three days. Because of their frequent replication, mutations in the DNA of colon cells can result in the formation of cancerous cells much more quickly. Curcumin also helps the body to destroy mutated cancer cells, and prevent the spreading of mutated cancer cell in the body. A primary way in which curcumin does so is by enhancing liver function. Additionally, other suggested mechanisms by which it may protect against cancer development include inhibiting the synthesis of a protein thought to be instrumental in tumor formation and preventing the development of additional blood supply necessary for cancer cell growth.[75-76]
Curcumin suppresses the growth of several tumor cell lines, including drug-resistant lines.
It suppresses the expression of cyclin D1, which is deregulated in a wide variety of tumors. Cyclin D1 is a component subunit of cyclin-dependent kinases (CDK) 4 (Cdk4) and 6 (Cdk6), which are rate limiting in progression of cells through the cell cycle. [77]
Curcumin also suppresses the activation of several transcription factors that are implicated in carcinogenesis.58 It suppresses the activation of nuclear factor kappa B (NF-_B). [78]
Curcumin suppresses the expression of TNF (TNF has been shown to mediate tumor initiation, promotion, and metastasis.) at both the transcriptional and posttranscriptional levels. Studies in our laboratory have shown that both TNF mRNA and protein are constitutively expressed in mantle cell lymphoma cell lines. [79-80]
Nagabhushan has shown that the curcumin in turmeric can: [81-85]
- inhibit the mutagenicity of polycyclic aromatic hydrocarbons (PAHs) (carcinogenic chemicals created by the burning of carbon based fuels including cigarette smoke)
- inhibit radiation-induced chromosome damage
- prevent the formation of harmful heterocyclic amines and nitroso compounds, which may result in the body when certain processed foods, such as processed meat products that contain nitrosamines, are eaten
- irreversibly inhibit the multiplication of leukemia cells in a cell culture
Use of Curcumin with Standard Oncologic Therapeutics:
1) Curcumin has been shown to augment the cytotoxic effects of chemotherapeutic drugs, including doxorubicin,tamoxifen. [86-87]
2) the combination of curcumin with cisplatin resulted in synergistic antitumor activity in the hepatic cancer HA22T/VGH cell line. [88]
LACK OF ANTIOXIDANT THERAPY:
The role and quantified level of consumed dietary antioxidants by individual patients as contained in fruits, vegetables, and grains, have not been viewed as an issue with respect to a patient’s response to anticancer drugs. [89-90]
Conclusions:
There is a concern that antioxidants might reduce oxidizing free radicals created by radiotherapy and some forms of chemotherapy, and thereby decrease the effectiveness of the therapy. animal and human studies demonstrate no reduction of efficacy of chemotherapy or radiation when given with antioxidants. In fact, considerable data exists showing increased effectiveness of many cancer therapeutic agents, as well as a decrease in adverse effects, when given concurrently with antioxidants.
References:
1. (J. Nutr. 134: 3479S–3485S, 2004)
2. Halliwell B and Aruoma OI. (eds) DNA and Free Radicals,Boca Raton Press, 1993.]
3. Blot WJ, Li JY, Taylor PR, et al. Nutrition intervention trials in Linxian, China: supplementation with specific vitamin/mineral combinations, cancer incidence, and disease-specific mortality in the general population. J Natl Cancer Inst 1993;85:1483–91.
4. The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. The effects of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med 1994;330:1029–35
5. Klaunig JE, Kamendulis LM Annu Rev Pharmacol Toxicol. 2004; 44():239-67
6. Dizdaroglu M, Jaruga P, Birincioglu M, Rodriguez HFree Radic Biol Med. 2002 Jun1;32(11):1102-15
7. Ames BN, Shigenaga MKAnn N Y Acad Sci. 1992 Nov 21; 663():85-96
8. Dreher D, Junod AF Eur J Cancer. 1996 Jan; 32A(1):30-8
9. cancer.gov/clinicaltrials.
10. clinicaltrials.gov
11. projectreporter.nih.gov/reporter.cfm
12. Cameron E, Pauling LC . 1979 Cancer and vitamin C. Philadelphia, PA:Camino Books.]
13. Bjelakovic G, Nikolova D, Gluud L, Simonetti R, Gluud C. 2007Mortality in randomized trials of antioxidant supplements for primary and secondary prevention. JAMA 297, 842–857.
14. royalsociety.org/news/2013/watson-antioxidants-cancer/
15. Conklin K. Dietary antioxidants during cancer chemotherapy: impact on chemotherapeutic effectiveness and development of side effects. Nutri Cancer 2000;37(1):1-18.
16. Han, R.M., Tian, Y.X., Becker, E.M., Andersen, M.L., Zhang, J.P., & Skibsted, L.H.(2007).Puerarin and conjugate bases as radical scavengers and antioxidants:molecular mechanism and synergism with beta-carotene. Journal of Agricultural and Food Chemistry, 0021-8561, Print, 1520-5118, Online, 55, 2384-2389.
17. Rivas, MA, Carnevale, R. P., Proietti, C. J., Rosemblit, C., Beguelin, W., Salatino, M.,Charreau, E. H., Frahm, I., Sapia, S., Brouckaert, P., Elizalde, P. V., & Schillaci, R. (2008). TNF alpha acting on TNFR1 promotes breast cancer growth via P42 P44 MAPK, JNK, Akt and NF-kappa B-dependent pathways. Experimental Cell Research, 314(3), 509-29, 0014-4827.
18. Q, & Kinneer, K. (2002) Chemoprotection by phenolic antioxidants. Inhibition of tumor necrosis factor alpha induction in macrophages. Journal of Biological Chemistry, 0021-9258, Print, 1083-351X, Online, 277, 2477-2484
19. Chen, L, Hu, JY, & Wang, SQ. (2012). The role of antioxidants in photoprotection: A critical review. Journal of the American Academy of Dermatology, 10.1016/j.jaad. 2012.02.009, [Epub ahead of print], 0190-9622, 0190-9622.
20. [ Formica JV, Regelson W Food Chem Toxicol. 1995 Dec; 33(12):1061-80]
21. [Altern Med Rev 2000]
22. Weast RC. Handbook of Chemisoy and Physics, 60th ed. CRC, Boca Raton, FL: 1979.
23. 23 Windholz M. The Merck Index. 10th ed Merck and Company, Rahway, NJ: 1983, pp. 1160.
24. Griffith JQ, Kreivson CF, Naghski J. Rutin and Related Flavonoids, 1955;234-42.
25. Mack Easton PA, Shakhova MK, Samokhvalov GI, Preobrazhenskii NA. Synthetic investigations in the field of flavonoids. Total synthesis of quercetin-3-,9-rutinoside, rutin. Zh. Obshch. Khim. (USSR), 1962;32:390-6.
26. Kuhnau J. The flavonoids. A class of semi-essential food components: Their role in human nutrition. World Rev. Nun: Diet. 1976;24:117-91.
27. Tamura G, Gold C, Ferro-Luzzi A, Ames BN. Fecalase: A model for activation of dietary glycosides to mutagens by intestinal floraRoc. NatL Acad Sci USA, 1980;77:4961-5.
28. Bokkenheuser VD, Shackleton CHL, Winter J. Hydrolysis of dietary flavonoids glycosides by strains of intestinal Bacteroides from humans. Biochem. J.1987;248:953-6.
29. Hollman PCH, van Trijp JMP, Mengelers MJB, et al. Bioavailability of the dietary antioxidant flavonol quercetin in man. Cancer Lett 1997;114:139-140
30. [Hollman PC, Katan MBBiomed Pharmacother. 1997; 51(8):305-10.]
31. Hollman PCH et al. Bioavailability of the dietary antioxidant flavonol quercetin in man. Cancer Letters, 1997;114:139-40.
32. Sakanashi Y et al. Possible use of quercetin, an antioxidant, for protection of cells suffering from overload of intracellular Ca2+: a model experiment. Life Sciences,2008;83:164-9.
33. Wiseman H, Halliwell B. Damage to DNA by reactive oxygen and nitrogen species : role ininflammatory disease and progression to cancer, Biochem. J, 1996;313:17-29.
34. Avila MA, Velasco JA, Cansado J, Notario V. Quercetin mediates the downregulation of mutant p53 in the human breast cancer cell line MDA-MB468. CancerRes, 1994;54:2424-8.
35. Hansen RK, Oesterreich S, Lemieux P, et al. Quercetin inhibits heat shock protein induction but not heat shock factor DNA-binding in human breast carcinoma cells. Biochem Biophys Res Commun 1997;239:851-856.
36. Elia G, Amici C, Rossi A, Santoro MG. Modulation of prostaglandin A1-induced thermotolerance by quercetin in human leukemic cells: role of heat shock protein 70. Cancer Res 1996;56:210-217.
37. Koishi M, Hosokawa N, Sato M, et al. Quercetin, an inhibitor of heat shock protein synthesis, inhibits the acquisition of thermotolerance in a human colon carcinoma cell line. Jpn J Cancer Res 1992;83:1216-1222
38. Yoshida M, Yamamoto M, Nikaido T. Quercetin arrests human leukemic T-cells in late G1phase of the cell cycle. Cancer Res, 1992;52:6676-81.
39. Ferry DR, Smith A, Malkhandi J, et al. Phase I clinical trial of the flavonoid quercetin: pharmacokinetics and evidence for in vivo tyrosine kinase inhibition. Clin Cancer Res, 1996;2:659-68.
40. Levy J, Teuerstein I, Marbach M, et al. Tyrosine protein kinase activity in the DMBAinduced rat mammary tumor: inhibition by quercetin. Biochem Biophys Res Commun 1984;123:1227-1233.
41. Boutin JA. Tyrosine protein kinase inhibition and cancer. Int J Biochem 1994;26:1203-1226.
42. Scambia G, Ranelletti FO, Benedetti Panici P et al. Quercetin induces type-II estrogenbinding sites in estrogen-receptor-negative (MDA-MB231) and estrogenreceptor- positive (MCF-7) human breast cancer cell lines. Int J Cancer, 1993;54:462-6.
43. Piantelli M, Maggiano N, Ricci R et al. Tamoxifen and quercetin interact with type II estrogen binding sites and inhibit the growth of human melanoma cells. J Invest Dermatol 1995;105:248-53.
44. Markaverich BM, Roberts RR, Alejandro MA, et al. Bioflavonoid interaction with rat uterine type II binding sites and growth inhibition. J Steroid Biochem 1988;30:71-78.
45. Rozenfel’d LG, Abyzov RA, Bozhko GT, et al. The possibilities of protection against local radiation injuries in ORL-oncologic patients. Vestn Otorinolaringol 1990;2:56-58. [Article in Russian].
46. Hofmann J, Fiebig HH, Winterhalter BR, et al. Enhancement of the antiproliferative activity of cis-diamminedichloroplatinum(II) by quercetin. Int J Cancer 1990;45:536-539.
47. Scambia G, Ranelletti FO, Panici PB, et al. Inhibitory effect of quercetin on primary ovarian and endometrial cancers and synergistic activity with cis-diamminedichloroplatinum (II). Gyn Oncol 1992;45:13-19.
48. . Kuhlman MK, Horsch E, Burkhardt G, et al.Reduction of cisplatin toxicity in cultured renal tubular cells by the bioflavonoid quercetin. Arch Toxicol 1998;72:536-540.
49. Hofmann J, Doppler W, Jakob A, et al. Enhancement of the antiproliferative effect of cis-diamminedichloroplatinum(II) and nitrogen mustard by inhibitors of protein kinase C. Int J Cancer 1988;42:382-388.
50. Sliutz G, Karlseder J, Tempfer C, et al. Drug resistance against gemcitabine and topotecan mediated by constitutive hsp70 overexpression in vitro: implication of quercetin as sensitiser in chemotherapy. Br J Cancer 1996;74:172- 177..
51. National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand including Recommended Dietary Intakes. Canberra, Australia, Commonwealth Department of Health and Ageing. 2006.
52. . Navarro Silvera SA, Rohan TE (2007) Trace elements and cancer risk: a review of the epidemiologic evidence. Cancer Causes Control 18: 7–27. doi: 10.1007/s10552-006-0057-z.
53. 53 Selenius, M., Rundlöf, A., Olm, E., Fernandes, A.P. & Björnstedt, M. (2010). Selenium and the Selenoprotein Thioredoxin Reductase in the Prevention, Treatment and Diagnostics of Cancer, Antioxidants & Redox Signaling 12(7): 867-880.
54. Almondes, K.G.S., Leal, G.V.S., Cozzolino, S.M.F.; Philippi, S.T. & Carvalho, P.H.R. (2010). O papel das selenoproteínas no câncer, Rev Assoc Med Bras 56(4): 484-488.
55. Lippman SM, Klein EA, Goodman PJ, Lucia MS, Thompson IM, et al. (2009) Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). Jama 301: 39–51. Doi.
56. Karunasinghe N, Ryan J, Tuckey J, Masters J, Jamieson M, Clarke LC, Marshall JR & Ferguson LR (2004) DNA stability and serum selenium levels in a high-risk group for prostate cancer. Cancer Epidemiology Biomarkers and Prevention 13, 391–397.
57. Kowalska E, Narod SA, Huzarski T, Zajaczek S, Huzarska J, Gorski B & Lubinski J (2005) Increased rates of chromosomebreakage in BRCA1 carriers are normalized by oral seleniumsupplementation. Cancer Epidemiology Biomarkers andPrevention 14, 1302–1306.
58. Waters DJ, Shen S, Glickman LT, Cooley DM, Bostwick DG, Qian J, Combs GF Jr & Morris JS (2005) Prostate cancer risk and DNA damage: translational significance of selenium supplementation in a canine model. Carcinogenesis 26, 1256–1262.
59. Ip C & Lisk DJ (1997) Modulation of phase I and phase II xenobiotic-metabolizing enzymes by selenium-enriched garlic in rats. Nutrition and Cancer 28, 184–188.
60. Smith ML, Lancia JK, Mercer TI & Ip C (2004) Selenium compounds regulate p53 by common and distinctive mechanisms. Anticancer Research 24, 1401–1408.
61. Myers C, Katki A, Travis E. Effect of tocopherol and selenium on defenses against reactive oxygen species and their effect on radiation sensitivity. Ann NY Acad Sci 1982;393:419-425.
62. Naganuma A, Satoh M, Imura N. Effect of selenite on renal toxicity and antitumor activity of cis-diamminedichloroplatinum in mice inoculated with ehrlich ascites tumor cell. J Pharm Dyn 1984;7:217-220.
63. Kappus H, Reinhold C. Inhibition of bleomycin-induced toxic effects by antioxidants in human malignant melanoma cells. Adv Exp Med Biol 1990;264:345-348.
64. Jensen, S.K. & Lauridsen, C. (2007). Alpha-tocopherol stereoisomers, Vitam Horm 76: 281-308.
65. Hahn, T., Szabo, L., Gold, M., Ramanathapuram, L., Hurley, L.H. & Akporiaye, E.T. (2006). Dietary Administration of the Proapoptotic Vitamin E Analogue Tocopheryloxyacetic Acid Inhibits Metastatic Murine Breast Cancer, Cancer Res 66: 9374-9378.
66. Turley JM, Funakoshi S, Ruscetti FW, et al. Growth inhibition and apoptosis of RL human B lymphoma cells by vitamin E succinate and retinoic acid: role for transforming growth factor beta. Cell Growth Differ 1995;6:655-663.
67. Pace, A., Savarese, A., Picardo, M., Maresca, V., Pacetti, U., Del Monte, G., Biroccio, A., Leonetti, C., Jandolo, B., Cognetti, F. & Bove, L. (2003). Neuroprotective Effect of Vitamin E Supplementation in Patients Treated With Cisplatin Chemotherapy, Journal of Clinical Oncology 21(5): 927-931.
68. Elattar TMA, Virji AS. Biphasic action of vitamin E on the growth of human oral squamous carcinoma cells. Anticancer Res 1999;19:365-368.
69. Kelloff GJ, Crowell JA, Boone CW. Clinical development plan: vitamin E. J Cell Biochem Suppl 1994;20:282-299.
70. . Bendich A, Machlin LJ. Safety of oral intake of vitamin E. Am J Clin Nutr 1988;48:612-619.
71. Alternative Medicine Review Volume 4, Number 5 1999 Page 313.
72. Chinery R, Brockman JA, Peeler MO, et al. Antioxidants enhance the cytotoxicity of chemotherapeutic agents in colorectal cancer: a p53-independent induction of p21 via C/ EBP-beta. Nat Med 1997;3:1233-1241.
73. Myers CE, McGuire WP, Liss RH, et al. Adriamycin: the role of lipid peroxidation in cardiac toxicity and tumor response. Science 1977;197:165-167.
74. Sakamoto K, Sakka M. Reduced effect of irradiation on normal and malignant cells irradiated in vivo in mice pretreated with vitamin E. Br J Radiology 1973;46:538-540.
75. Ahsan H, Parveen N, Khan NU, Hadi SM. Pro-oxidant, anti-oxidant and cleavage activities on DNA of curcumin and its derivatives demethoxycurcumin and bisdemethoxycurcumin. Chem Biol Interact 1999 Jul 1;121(2):161-75. 1999. PMID:7690
76. Tayyem RF, Heath DD, Al-Delaimy WK, Rock CL. Curcumin content of turmeric and curry powders. Nutr Cancer. 2006;55(2):126-31. 2006. PMID:17044766.
77. Mukhopadhyay A, Banerjee S, Stafford LJ, Xia C, Liu M, Aggarwal BB. Curcumin-induced suppression of cell proliferation correlates with down-regulation of cyclin D1 expression and CDK4-mediated retinoblastoma protein phosphorylation. Oncogene 2002;21(57):8852-61.
78. Aggarwal BB, Kumar A, Bharti AC. Anticancer potential of curcumin: preclinical and clinical studies. Anticancer Res 2003;23(1A):363-98.
79. Shishodia S, Amin HM, Lai R Aggarwal BB. Curcumin (diferuloylmethane) inhibits constitutive NF-kappaB activation, induces G1/S arrest, suppresses proliferation, and induces apoptosis in mantle cell lymphoma. Biochem Pharmacol 2005;70(5):700-13
80. Aggarwal BB. Signalling pathways of the TNF superfamily: a double-edged sword. Nat Rev Immunol 2003;3(9):745-56.
81. Nagabhushan M, Amonkar AJ, Bhide SV. In vitro antimutagenicity of curcumin against environmental mutagens. Food Chem Toxicol. 1987 Jul;25(7):545-7. 1987. PMID:3623345.
82. Nagabhushan M, Bhide SV. Curcumin as an inhibitor of cancer. J Am Coll Nutr. 1992 Apr;11(2):192-8. 1992. PMID:1578097.
83. Nagabhushan M, Nair UJ, Amonkar AJ, D'Souza AV, Bhide SV. Curcumins as inhibitors of nitrosation in vitro. Mutat Res. 1988 Nov;202(1):163-9. 1988. PMID:3054526.
84. Nagabhushan M. Research presented at the Children with Leukaemia Conference, www.leukaemia.org, September 2004. 2004.
85. Nakamura K, Yasunaga Y, Segawa T et al. Curcumin down-regulates AR gene expression and activation in prostate cancer cell lines. Int J Oncol 2002 Oct;21(4):825-30. 2002.
86. Harbottle A, Daly AK, Atherton K, Campbell FC. Role of glutathione S-transferase P1, P-glycoprotein and multidrug resistance-associated protein 1 in acquired doxorubicin resistance. Int J Cancer 2001;92(6):777-83.
87. Verma SP, Goldin BR, Lin PS. The inhibition of the estrogenic effects of pesticides and environmental chemicals by curcumin and isoflavonoids. Environ Health Perspect 1998;106(12):807-12.
88. Notarbartolo M, Poma P, Perri D, Dusonchet L, Cervello M, D’Alessandro N. Antitumor effects of curcumin, alone or in combination with cisplatin or doxorubicin, on human hepatic cancer cells. Analysis of their possible relationship to changes in NF-kB activation levels and in IAP gene expression. Cancer Lett 2005;224(1):53-65.
89. Kelloff GJ. Perspectives in cancer prevention In: Vanderwoude GF, Klein G, eds Research and Drug Development Advances in Cancer Research. London: Academic Press; 2000:199-334.
90. Hong WK, Spitz MR, Lippman SM. Cancer chemoprevention in the 21st century: genetics, risk modeling, and molecular targets. J Clin Oncol. 2000;(suppl)18:9S-18S.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






