

About Authors:
Sandhu Premjeet1, 2,Rathore Devashish2, Kataria Sahil1 , Middha Akanksh1
1Seth G. L. Bihani S.D. College of Technical Education,
Institute of Pharmaceutical Sciences and Drug Research,
Sri Ganganagar, Rajasthan, INDIA
2 School of Pharmaceutical Sciences, RGPV University campus,
Bhopal, M.P, INDIA
ABSTRACT
The blood – brain barrier (BBB) has always presented a challenge to scientists for brain drug targeting . the BBB evolved in such a way that it protects the brain from various foreign substance such as neurotoxins. This mechanism makes the BBB an insurmountable . This mechanism makes BBB an insurmountable barrier for numerous highly essential drugs , including antibiotics, cytostatics and other CNS active drug Drugs may be administered directly into the CNS or administered systematically (e.g. by intravenous injection) for targeted action in the CNS. The major challenge to CNS drug delivery is the blood-brain barrier (BBB), which limits the access of drugs to the brain substance. Various strategies that have been used for manipulating the blood-brain barrier for drug delivery to the brain include osmotic and chemical opening of the blood-brain barrier as well as the use of transport/carrier systems. Other strategies for drug delivery to the brain involve bypassing the BBB. Various pharmacological agents have been used to open the BBB and direct invasive methods can introduce therapeutic agents into the brain substance. It is important to consider not only the net delivery of the agent to the CNS, but also the ability of the agent to access the relevant target site within the CNS. Various routes of administration as well as conjugations of drugs, e.g. with liposomes and nanoparticles are considered. Some routes of direct administration to the brain are non-invasive such as transnasal route whereas others involve entry into the CNS by devices and needles such as in case of intrathecal and intracerebroventricular delivery.
[adsense:336x280:8701650588]
Reference ID: PHARMATUTOR-ART-1188
INTRODUCTION
Most conventional dosage form deliver drug into the body that eventually reaches the site of action by distribution and passive diffusion . The drug also distribute to non targeted site tissues because of nonselective distribution a much larger dose is given to the patient to achive therapeutic concentration into the desired tissue. However drug action at the nontarget sites may result in toxicity or other adverse reaction. Delivery system that target the drug only to the desired site of drug action allow for more selective and targeted drug therapy could result in a significant reduction on dose and cost.
Targeted drug delivery is a method of delivering medication to a patient in a manner that increases the concentration of the medication in some parts of the body relative to others. In traditional drug delivery systems such as oral ingestion or intravascular injection, the medication is distributed throughout the body through the systemic blood circulation. For most therapeutic agents, only a small portion of the medication reaches the organ to be affected. This improves efficacy of the while reducing side effects. There are two kinds of targeted drug delivery, active targeted drug delivery, such as some antibody medications; and passive targeted drug delivery, such as the Enhanced Permeability and Retention effect3.
BRAIN DRUG TARGETING
The brain is a delicate organ, and evolution built very efficient way to protect it .Unfortunately , the same mechanism that protect it against intrusive chemicals also frustrate therapeutic interventions. Many existing pharmaceutical are rendered ineffective in the treatment of cerebral diseases due to inability to effectively deliver and sustain them with them within brain. Various strategies that have been used for manipulating the blood-brain barrier for drug delivery to the brain include osmotic and chemical opening of the blood-brain barrier as well as the use of transport/carrier systems. Other strategies for drug delivery to the brain involve bypassing the BBB. Various pharmacological agents have been used to open the BBB and direct invasive methods can introduce therapeutic agents into the brain substance. It is important to consider not only the net delivery of the agent to the CNS, but also the ability of the agent to access the relevant target site within the CNS.
Various routes of administration as well as conjugations of drugs, e.g. with liposomes and nanoparticles, are considered. Some routes of direct administration to the brain are non-invasive such as transnasal route whereas others involve entry into the CNS by devices and needles such as in case of intrathecal and intracerebroventricular delivery. Systemic therapy by oral and parenteral routes is considered along with sustained and controlled release to optimize the CNS action of drugs. Among the three main approaches to drug delivery to the CNS systemic administration, injection into CSF pathways, and direct injection into the brain - the greatest developments is anticipated to occur in the area of targeted delivery by systemic administration. Cell, gene and antisense therapies are not only innovative treatments for CNS disorders but also involve sophisticated delivery methods. RNA interference (RNAi) as a form of antisense therapy is also described. The role of drug delivery is depicted in the background of various therapies for neurological diseases including drugs in development and the role of special delivery preparations. Pain is included as it is considered to be a neurological disorder.
[adsense:468x15:2204050025]
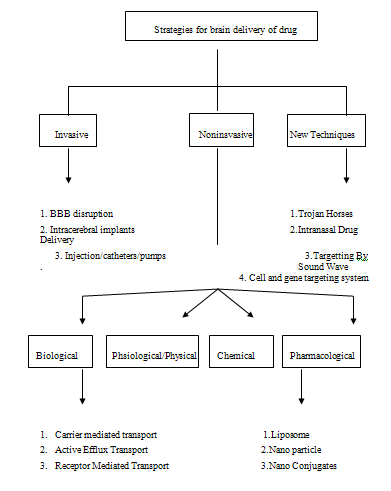
INVASIVE STRATEGIES FOR BRAIN TARGETTING
Temporary physiological distruption of endothelial integrity of the brain is one of the invasive strategies for drug delivery to the brain . Hypertonic distruption with help of 25% mannitol or arabinose enhances the delivery of the small molecular weight cytostatic agent to the brain tumours. Osmotic distruption has been tested as a strategy for the drain delivery of macromolecular drugs such as monoclonal antibodies nanoparticle and viruses. BBB opening also achieved by the receptor mediated mechanism. Vasoactive compounds like prostaglandin, histamine, serotonine and leukotrine havs all been shown to induce BBB leakage12.
Disruption of the BBB
The thought behind this approach was to break down the barrier momentarily by injecting mannitol solution into arteries in the neck. The effect lasts for 20-30 minute, during which time drugs diffuse freely, that would not normally cross the BBB. This method permitted the delivery of chemotherapeutic agents in patients with cerebral lymphoma, malignant glioma and disseminated CNS germ cell tumors. Physiological stress, transient increase in intracranial pressure, and unwanted delivery of anticancer agents to normal brain tissues are the undesired side-effects of this approach in humans11.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Variuos Techniques of Drug Delivery to Brain
Osmotic Blood-Brain Barrier Disruption
In the search for treatment of patients with rapidly growing, high grade gliomas, osmotic opening of the BBB was developed. Intracarotid injection of an inert hypertonic solution such as mannitol or arabinose has been employed to initiate endothelial cell shrinkage and opening of BBB tight junctions for a period of a few hours, and this permits delivery of antineoplastic agents to the brain. Although controversial, the method has shown promise in augmenting delivery of neurotoxic drugs to the CNS. However, some glial tumors have an endothelial barrier which is compromised, probably because the glial production of barrier-inducing factors is altered. For this reason, osmotic opening used in conjunction with cytotoxic drugs (such as carboplatin) may give an advantage over traditional chemotherapy. Osmotic disruption seems to be most successful in treating primary non-AIDS CNS lymphoma. The chemical induction of fenestrated capillaries is attributed to the production of the plasminogen activator urokinase, and is completely reversed 1-2 months after delivery of retinoic acid or PMA is stopped. Osmatic distruption also has been tested as a strategy for the delivery of macromolecular drugs such as monocolonal antibodies, nanoparticles and viruses.
Biochemical Blood-Brain Barrier Disruption
Recently, new and potentially safer biochemical techniques have been developed to disrupt the BBB. Selective opening of brain tumor capillaries (the blood-tumor barrier), by the intracarotid infusion of leukotriene C4 was achieved without concomitant alteration of the adjacent BBB. In contrast to osmotic disruption methods, biochemical opening utilizes the novel observation that normal brain capillaries appear to be unaffected when vasoactive leukotriene treatments are used to increase their permeability. The mechanism was shown to be related to the abundance of g-glutamyl transpeptidase (g-GTP) in normal brain capillaries; this enzyme requires glial inductive influence for its expression, and it is down- regulated in tumors, resulting in a reduction of the enzymatic barrier in tumor endothelial cells.
INTRACEREBRAL IMPLANTS
Intracerebral chemotherapy delivery by polymeric implants increase survival of humans with recurrent malignant gilomas and of animal with transplanted gilomas. Drug added to polymer pellets implants intracranically bypass the BBB and release drug molecules locally in the brain in a sustained fashion . Malignant gilomas are deeply in the brain and thus the effectiveness of brain delivery by the polymers is dependent on whether drug molecules can be transported a sufficient distance from the implanted site reach malignant gilomas. The polymer implants substance designed to treat tumor can be administered directly to the affected area of the brain and release in a sustained manner for a long period of time12.
INTRAVENTRICULAR/INTRATHECAL ROUTE
One strategy for bypassing the BBB that has been studied extensively both in laboratory and in clinical trials is the intralumbar injection or intreventricular infusion of drugs directly into the CSF. Drugs can be infused intraventricularly using an Ommaya reservoir, a plastic reservoir implanted subcutaneously in the scalp and connected to the ventricles within the brain via an outlet catheter. Drug solutions can be subcutaneously injected into the implanted reservoir and delivered to the ventricles by manual compression of the reservoir through the scalp.
When compared to vascular drug delivery, intra-CSF drug administration theoretically has several advantages. Intra-CSF administration bypasses the BCB and results in immediate high CSF drug concentrations. Since, the drug is somewhat contained within the CNS, a smaller dose can be used, potentially minimizing systemic toxicity. Furthermore, drugs in the CSF encounter minimized protein binding and decreased enzymatic activity relative to drugs in plasma, leading to longer drug half-life in the CSF. Finally, because the CSF freely exchanges molecules with the extracellular fluid of the brain parenchyma, delivering drugs into the CSF could theoretically result in therapeutic CNS drug concentrations.
INJECTIONS, CATHETERS, AND PUMPS
Several techniques have been developed for delivering drugs directly to the brain interstitium. One such methodology is the Ommaya reservoir or implantable pump as discussed earlier under intraventricular/intrathecal route. This technique, however, does achieve truly continuous drug delivery. More recently, several implantable pumps have been developed that possess several advantages over the Ommaya reservoir. This can be implanted subcutaneously and refilled by subcutaneous injection and are capable of delivering drugs as a constant infusion over an extended period of time. Furthermore, the rate of drug delivery can be varied using external handheld computer control units. Currently each of the three different pumps available for interstitial CNS drug delivery operates by a distinct mechanism. The Infusaid pump uses the vapour pressure of compressed Freon to deliver a drug solution at a constant rate; the MiniMed PIMS system uses a solenoid pumping mechanism, and the Medtronic SynchroMed system delivers drugs via a peristaltic mechanism. Another recent study shows that the epidural (EPI) delivery of morphine encapsulated in multivesicular liposomes (DepoFoam drug delivery system) produced a sustained clearance of morphine and a prolonged analgesia, and the results suggest that this delivery system is without significant pathological effects at the dose of 10mg/ml morphine after repeated epidural delivery in dogs7.
2. NONINVASIVE STRATEGIES
Non-invasivewhen no break in the skin is created and there is no contact with the mucosa, or skin break, or internal body cavity beyond a natural or artificial body orifice. the first modern non-invasive techniques based on physical methods, electrocardiography and X-rays,. Non-invasive techniques commonly used for Gene expression imaging, ultrasonographyand echocardiography using ultrasoundwaves for imaging.
BIOLOGICAL DELIVERY
The biology-based approaches require prior knowledge of the endogenous transport systems within the brain capillary endothelium, which forms the BBB in vivo. The biology-based strategies for brain drug delivery are founded on the principle that there are numerous endogenous transport systems within the BBB, and that these transporters are conduits to the brain. The endogenous BBB transport systems may be broadly classified as carrier-mediated transport (CMT), active efflux transport (AET), and receptor-mediated transport (RMT)
a. BBB Carrier-Mediated Transport
The conversion of dopamine, a water-soluble catecholamine that does not cross the BBB, into the corresponding α -amino acid, l-DOPA, enables dopamine delivery to the brain, which has been the mainstay of treatment of PD for nearly 40 years . The use of l-DOPA to deliver dopamine to the brain is a BBB drug-delivery strategy that utilizes the type 1 large neutral amino acid transporter (LAT1)—one of the CMT systems within the BBB. Upon crossing the BBB through LAT1, l-DOPA is converted back to dopamine within the brain by aromatic amino acid decarboxylase (AAAD). Other drugs that cross the BBB via LAT1 include melphalan for brain cancer, α -methyl-DOPA for treatment of high blood pressure, and gabapentin for epilepsy . Apart from LAT1, there are other BBB CMT systems that could be accessed to solve BBB drug-delivery problems , including the GLUT1 glucose transporter, the MCT1 lactate transporter, the CAT1 cationic amino acid transporter, and the CNT2 adenosine transporter, among others. If the BBB CMT systems are to be exploited to overcome the BBB drug-delivery problem, the drug must be reformulated such that the drug assumes a molecular structure mimicking that of the endogenous ligand. This principle is illustrated by gabapentin, which is 1-(aminoethyl) cyclohexaneacetic acid. Gabapentin is a γ -amino acid, not an α -amino acid. However, this drug’s structure does mimic that of an α -amino acid and is recognized by the BBB LAT1 large neutral amino acid transporter. In the absence of LAT1-mediated transport across the BBB, gabapentin would be too water soluble to cross (via lipid mediation) the BBB in pharmacologically significant amounts.
b. BBB ActiveEffluxTransport
P-glycoprotein (Pgp) is the prototypic AET system found at the BBB. However, there are many other AETs other than Pgp that function at the BBB to cause the selective export of metabolites from brain back to blood. Although Pgp is principally expressed at the capillary endothelium in rodent brains, this transporter is also expressed at both the capillary endothelium and at astrocyte processes in primate and human brains ). Within the brain capillary endothelium, it is assumed that Pgp is selectively localized at the luminal membrane, although the definitive immunogold electron-microscopic studies for this transporter have yet to be performed for brain.
c. BBB Receptor-MediatedTransport
Certain endogenous large-molecule neuropeptides such as insulin, transferrin, or leptin access the brain from blood via receptor-mediated transport (RMT) across the BBB (Figure 4). This transport is mediated by specialized ligand-specific receptor systems, including the insulin receptor (IR) or the transferrin receptor (TfR), which are highly expressed on the capillary endothelium of brain . Certain peptidomimetic monoclonal antibodies (MAbs) bind to exofacial epitopes on the BBB receptors. These epitopes are spatially separated from the endogenous ligand-binding site, and the binding of MAbs to the BBB receptor enables RMT of the peptidomimetic MAb across the BBB in vivo. These peptidomimetic MAbs may be used as “molecular Trojan horses” to ferry large-molecule drugs (e.g. recombinant proteins, gene-based medicines) across the BBB
2.2 PHYSIOLOGICAL/PHYSICAL STRATEGIES
The above strategies are primarily aimed at short term application in the treatment regiments of malignant brain tumors while chronic degrative disorder will require long term application of the therapeutic agent . owing to this fact non invasive approach for the drug delivery to brain via the systemic route have been developed .
LIGAND BINDING PROTEIN
Protein ligands posses various properties like high affinity to receptor and selectivity for targeting , which increase the interst towards the use of protein as a delivery tool for targeting the drug to the brain. Various system have been developed that incorporate proteing as the central ligand binding component such as lecitin used as a ligand bunding protein for brain targeting of glucose triggered glycosylated insulin and bispecific antibodies. Other ligand binding protein classes include biotin binding protein. Lipid binding protein and avidin binding proteins. Cationized albumin appers to be useful for the delivery of the active agents across the BBB to the brain . The active agents across the BBB to the brain.
CHIMERIC PEPTIDE
A new strategy for peptide delivery through the brain capillary wall, i.e., the blood-brain barrier (BBB), is the synthesis of chimeric peptides which are formed by the covalent coupling of a non-transportable peptide (e.g., β-endorphin) to a transportable peptide that undergoes receptor- or absorptive-mediated transcytosis at the BBB. β-endorphin was covalently coupled via disulfide linkage to cationized albumin (pI ≥ 9) which, owing to it is highly basic charge, undergoes rapid absorptive-mediated transport into brain from blood. (http://www.sciencedirect.com/science)
2.3 CHEMICAL DRUG DELIVERY
Chemical drug delivery systems (CDDS) represent novel and systematic ways of targeting active biological molecules to specific target sites or organs based on predictable enzymatic activation. They are inactive chemical derivatives of a drug obtained by one or more chemical modifications so that the newly attached moieties are monomolecular units (generally comparable in size to the original molecule) and provide a site-specific or site-enhanced delivery of the drug through multi-step enzymatic and/or chemical transformations. During the chemical manipulations, two types of bio-removable moieties are introduced to convert the drug into an inactive precursor form. A targetor (T) moiety is responsible for targeting, site-specificity, and lock-in, while modifier functions (F1... Fn ) serve as lipophilizers, protect certain functions, or fine-tune the necessary molecular properties to prevent premature, unwanted metabolic conversions. The CDDS is designed to undergo sequential metabolic conversions, disengaging the modifier functions and finally the targetor, after this moiety fulfils its site- or organ-targeting role. Undoubtedly, the concept evolved from the prodrug concept, but became essentially different by the introduction of multi-step activation and targetor moieties. Another method called redox chemical delivery systems involves linking a drug to the lipophilic dihydropyridine carrier, creating a complex that after systemic administration readily transverses the BBB because of its lipophilicity. Once inside the brain parenchyma, the dihydropyridine moiety is enzymatically oxidized to the ionic pyridinium salt. The acquisition of charge has the dual effect of accelerating the rate of systemic elimination by the kidney and bile and trapping the drug-pyridinium salt complex inside the brain. Subsequent cleavage of the drug from the pyridinium carrier leads to sustained drug delivery in the brain parenchyma7.
2.4 PHARMACOLOGICAL STRATEGIES
a.LIPOSOMES :-
Liposomes were first produced in England in 1961 by Alec D.Bangham. One end of each molecule is water soluble, while the opposite end is water insoluble. Water-soluble medications added to the water were trapped inside the aggregation of the hydrophobic ends; fat-soluble medications were incorporated into the phospholipid layer.
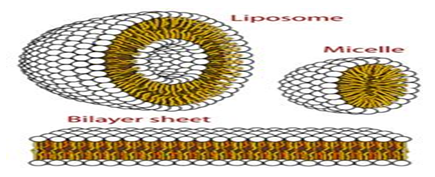
Liposome structure
In some cases liposomes attach to cellular membranes and appear to fuse with them, releasing their or drugs into the cell. In the case of phagocytic cells, the liposomes are taken up, the phospholipid walls are acted upon by organelles called lysosomes, and the medication is released. Liposomal delivery systems are still largely experimental; the precise mechanisms of their action in the body are under study, as are ways in which to target them to specific diseased tissues11.
Immunoliposomes (antibody-directed liposomes) were used in the present study for delivery of the antineoplastic agent daunomycin to the rat brain. A coupling procedure was introduced, which allows conjugation of a thiolated antibody to maleimide-grafted 85-nm liposomes sterically stabilized with PEG. Antibody was thereby coupled to the terminal end of a PEG-conjugated linker lipid. No brain uptake of PEG-conjugated liposomes carrying [3H]daunomycin was observed. However, brain targeting of immunoliposomes carrying [3H]daunomycin was mediated by the OX26 monoclonal antibody to the rat transferrin receptor, which is selectively enriched at the brain microvascular endothelium that comprises the blood–brain barrier in vivo.
First, PEG-conjugated immunoliposomes were synthesized using thiolated mAb and a bifunctional 2000-Da PEG (PEG) that contains a lipid at one end and a maleimide at the other end. Second, the pharmacokinetics and brain uptake of [3H]daunomycin was examined following intravenous administration of the drug in free form, as a conventional liposome, as a PEG-conjugated liposome, and as a PEG-conjugated immunoliposome. The mAb used in these studies is the OX26 mAb to the rat transferrin receptor , which is abundant on brain microvascular endothelium.
2.4(b) Nanoparticulate systems for brain delivery of drugs(Nanotechnology)
One of the possibilities to deliver drugs to the brain is the employment of nanoparticles.Nanopartiacles are polymeric particles made of natural or artificial polymers ranging in size between about 10 and 1000 nm (1 mm). Drugs may be bound inform of a solid solution or dispersion or be adsorbed to the surface or chemically attached. Poly (butylcyanoacrylate) nanoparticles represent the onlynanoparticles that were so far successfully used for the in vivo delivery of drugs to the brain. The first drug that was de-livered to the brain usingnanoparticles was thehexapeptidedalargin (Tyr-D-Ala- Gly- Phe-Leu-Arg), aLeu-enkephalin analogue withopioid activity.
Nanoparticles andnanoformulations have already been applied as drug delivery systems with great success; andnanoparticulate drug delivery systems have still greater potential for many applications, including anti-tumors therapy, gene therapy, and AIDS therapy, radiotherapy, in the delivery of proteins, antibiotics,virostatics, and vaccines and as vesicles to pass the blood - brain barrier.
In some cases it is reported to mimic molecules that would normally be transported to brain. For example,polysorbate-coatednanoparticles are thought to mimic low-density lipoprotein (LDL), allowing them to be transported across the capillary wall and into the brain by hitchingaride on the LDL receptor .
The nanotechnology includes-
1) Coatednanoparticles
2)Pegylatednanoparticles
3)Solid Lipidnanoparticles (SLN)
4)Nanogels
Advantages of nanotechnology :-
1) Due to their small size nanoparticles penetrate into even small capillaries and are taken up within cells, allowing an efficient drug accumulation at the targeted sites in the body.
2) The use of biodegradable materials for nanoparticle preparation, allows sustained drug release at the targeted site after injection over a period of days or even weeks
Although the total drug-load is reduced considerably and the manufacture process is more complex, the nanoscale devices present some advantages over the micro-systems. In fact, submicron systems show higher intracellular uptake than microsized particles, thereby allowing drug-release in different cellular compartments such as cytoplasm and nucleus. Nanoparticles can be also easily conjugated with a ligand to favour a targeted therapeutic approach and as it has been reported, some nanoparticles can cross the blood-brain barrier (BBB). For example, doxorubicin bound to polysorbate-coated nanoparticles can cross the intact BBB, reaching therapeutic concentrations in the brain.
2.4(c) NANOCONJUGATES
These are low molecular weight conjugates of a small drug or toxin and a targeting ligand coupled through a cleavable linker group which is consisted of three functional domain , the targeting group, a linker , and an active agent / drug . typically nanoconjugates have a molecular weight similar to that of standard cyto toxic drugs .drug transport and distribution in the interstitial are based on convection and diffusion .The convection transport of molecules is independent of therir molecular weight carrying molecules in the flow of blood or interstitial fluid . solid tumours frequently have an increased interstitial pressure that severely limits convection based transport of drugs . the efficiency of drug transport through diffusion on the other hand is inversely proportional to the molecular weight of the drug/carrier . thus small molecules and nanoconjugates have potential advantages in situations where drug transport is diffusion limited.(Soni et al.2004)
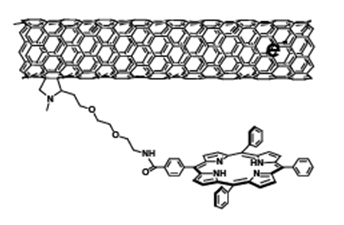
Figure : Nanoconjugate based endotoxin
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
3. New Techniques
3.1 Trojan horses Aproach in drug delivery to brain
Current CNS drug treatments predominantly address four CNS disorders: depression, schizophrenia, chronic pain and epilepsy, whereas treatment options for brain cancer, neurodegenerative diseases and most other CNS conditions are quite limited These limitations can be directly linked to the blood–brain barrier (BBB), a physical, metabolic and immunological barrier formed by endothelial cells, pericytes, astrocytes and the basal membrane. It controls the transport of molecules from the blood circulation to the brain parenchyma so effectively that around 95% of more than 7000 small bioactive compounds (MW<500) covered by the Comprehensive Medicinal Chemistry database (and 100% of large bioactive molecules) have insufficient bioavailability in the brain .
Under physiological conditions, control of transport across the BBB is achieved as follows:
a. minimization of transbarrier transport (for example, through continuous tight junctions, lack of fenestrations and minimal pinocytosis of brain endothelial cells);
b. active expulsion of the unwanted molecules that cross the barrier by efflux pumps (for example, P-glycoprotein (P-gp), members of the multi resistance protein family, organic anion and cation transporters) and
c. selective and active transport of the required substrates through a range of transporters and internalizing receptors.
Not surprisingly, delivery strategies to overcome the BBB utilize all of these mechanisms in an effort to increase CNS drug bioavailability , by increasing lipid diffusion , temporary opening of the barrier pharmacologically or through osmotic shock, by coadministration of chemotherapeutic agents with efflux pump inhibitors, or coupling of drugs and drug carriers to the endogenous substrates of various transporters/receptors or the corresponding antibodies (e.g. OX26).
In the case of Angiopep-2 such sites/functions might include the liver, where LRP1 serves as a hepatocyte receptor involved in the lipid metabolism, vascular smooth muscle cells, macrophages and but also the coagulation-fibrinolysis system . LRP2 on the other hand is also expressed on the apical plasma membrane of absorptive and secretory epithelia, as found in renal proximal tubules, thyroid and parathyroid glands, tropho-ectoderm and neuroectoderm . High levels of LRP-type receptors are also present on gliomas but it is currently unclear whether this may affect the pharmacology of ANG1005 .
It is now important to explore some of the remaining questions in more detail to determine whether ‘Trojan horse' systems such as ANG1005 will have a general role to play in CNS drug therapy or are more suited to specific ‘courses', i.e. selected drug/disease combinations1.
3.2 INTRANASAL DRUG DELIVERY TECHNIQUE
Nasal delivery drugs first reach the respiratory epithelium, where compounds can be absorbed into the systemic circulation by Tran cellular and Para cellular passive absorption, carrier-mediated transport, and absorption through trancytosis. When a nasal drug formulation is delivered deep and high enough into the nasal cavity, the olfactory mucosa may be reached and drug transport into the brain and/or CSF via the olfactory receptor neurons may occur11.
Intranasal Mucoadhesive Microemulsions of Sumatriptan
Migraine attack is a troublesome physiological condition associated with throbbing, intense headache in one-half of the head. During an attack, the blood vessels in the brain dilate and then draw together with stimulation of nerve endings near the affected blood vessels. These changes to the blood vessels and stimulation of nerves are probably what cause the pain, although migraine is still a poorly understood condition or phenomenon. Migraine treatment has evolved into the scientific arena, but opinions differ on whether migraine is primarily a vascular or a neurological dysfunction.
ST/SS, triptan derivatives are serotonin (5-hydroxytryptamine) agonists available in the market in oral tablets and subcutaneous injection dosage form for the treatment of migraine. ST is also available in a rectal suppository dosage form for the treatment of migraine attacks. A substantial proportion of migraine patients not only suffer from gastric stasis but also have severe nausea and vomiting, which results in erratic absorption of ST from the gastrointestinal tract. ST is rapidly but incompletely absorbed following oral administration and undergoes first-pass metabolism, resulting in a low absolute bioavailability of 14% in humans. Moreover, the transport of ST across the blood-brain barrier (BBB) is very poor, although evidence of detection of some drug in cerebrospinal fluid (CSF) following high IV dose has been cited in the literature.7Therefore, an alternative route of drug delivery that can selectively target the drug directly into various regions of the brain, including vasculature, is needed for the treatment of acute attacks of migraine8.
3.3 TARGETING THE BRAIN WITH SOUND WAVES
Ultrasound waves, currently used in medicine for prenatal scans and other diagnostic purposes, could one day be used as a noninvasive way to control brain activity. Over the past two years, scientists have begun experimenting with low-frequency, low-intensity ultrasound that can penetrate the skull and activate or silence brain cells. Researchers hope that the technology could provide an alternative to more-invasive techniques, such as deep-brain stimulation (DBS) and vagus nerve stimulation, which are used to treat a growing number of neurological disorders.
High intensityfocused ultrasound has already been approved to treat uterine fibroids and clinical trials for its use to destroy breast cancers and other tumors are underway. Treating the brain, however, requires a slightly different approach. The human skull acts as a shield, absorbing energy and distorting the path of waves including the sound waves found in ultrasound beams. Insightec solved this difficulty by designing a collection of over one thousand independently focusable transducers and placing them inside a helmet worn over the patient's head. The resulting level of control allows the operator to precisely compensate for the shielding effect, allowing the resulting beams to reach the desired location. A cooling system is also used to ensure the skull doesn't overheat during the procedure.
Real-time magnetic resonance imaging scans, better known as MRIs, are used to locate the desired focal point of the beams (which differs from patient to patient depending on their specific problem and their individual brain morphology) and to monitor their effectiveness. The beam heats the target area to 130 degrees Fahrenheit, hot enough to kill the cells within the affected 10 cubic millimeter volume.
With ultrasound, we have a much better spatial focus than [with] DBS,. And unlike TMS, we can get anywhere in the brain." Ultrasound--consisting of sound waves with a frequency above 20 kilohertz--has been used for decades in medicine to image muscle, organs, and fetuses. In the past five years, better tools for focusing ultrasound energy have enabled its use as an ablation tool: surgeons can now use high-intensity, high-frequency ultrasound (HIFU) to essentially burn away uterine fibroids. HIFU is also in clinical testing for treating brain tumors, breast tumors, and prostate cancer
These same tools are now allowing scientists to apply ultrasound to control the brain, an idea that has actually been around for decades. Better ultrasound transducers, which generate the acoustic waves, enable more-precise focusing of ultrasound energy. And magnetic resonance imaging (MRI) used in conjunction with ultrasound allows surgeons to target specific areas of the body more precisely. "The ability to marry focused ultrasound with MR [magnetic resonance] guidance is exceedingly powerful," a neurosurgeon at the University of Virginia, in Charlottesville, and chairman of the Focused Ultrasound Surgery Foundation, a nonprofit based in Charlottesville that was founded to develop new applications for focused ultrasound.(Emily el al 2009)
3.4 Cell and gene targeting systems
Brain drug targeting technology is based on the application of four gene technologies that enable the delivery of drugs or genes across the blood-brain barrier (BBB) in vivo. I) Genetic engineering is used to produce humanized monoclonal antibodies that target endogenous BBB transporters and act as vectors for delivery of drugs or genes to the human brain. The conjugate of a neurotherapeutic and a BBB transport vector is called a chimeric peptide. Epidermal growth factor chimeric peptides have been used for neuroimaging of brain cancer. Brain-derived neutrophic factor chimeric peptides have marked neuroprotective effects in brain stroke models. II) Imaging gene expression in the brain in vivo is possible with sequence-specific antisense radiopharmaceuticals, which are conjugated to BBB drug targeting vectors. III) Brain gene targeting technology enables widespread expression of an exogenous gene throughout the central nervous system following an intravenous injection of a non-viral therapeutic gene. IV) A BBB genomics program enables the future discovery of novel transport systems expressed at the BBB. These transporters may be carrier-mediated transport systems, active efflux transporters, or receptor-mediated transcytosis systems. The future discovery of novel BBB transport systems and the application of brain drug targeting technology will enable the delivery to the brain of virtually any neurotherapeutic, including small molecules, large molecules and gene medicines.
1.Avidin –biotin technology :
The conjugation of drugs to BBB transport vector is facilitated with used of avidin biotin technology . in this approacg , a genetically engineered fusion gene is constructed which enables production of a fusion protein compromised of the BBB transport vector and either avidin or streptavidin . alternatively chemical conjugation of the transport vector and avidin or SA is designated OX26/SA . in parallel the non transportable neurotherapeutic is monobiotinylated. Owing to the extremely high affinity of SA binding of biotin there is instantaneous formation of the conjugate upon mixing of the monobiotinylated therapeutic with the MAb/SA . in this 2vial approach to pharmaceutical formulation the biotinylated neurotherapeutic is prepared in one vial , the MAb/SA is prepared in a second vial , and the two vials are mixed , just prior to administration , resulting in a rapid formation of the drug –biotin /SA-MAb conjugate.
2.Genetically engineered monoclonal antibodies for human therapy-
the immunogenecity of the MAb was eliminated with genetic engineering and formation of a chimeric HIRMAb , the chimeric HIRMAb retained 100% affinity for the HIR following genetic engineering based on both western blot analysis and quantitative ELISA. Genetically engineered chimeric HIRMAb was conjugated with DTPA for labeling with 111-indium. . the availability of genetically engineered BBB transport vectors that are highly active in humans means that it is now possible to deliver to the brain protein therapeutic .
3.Brain targeting of protein therapeutic to brain with the chimeric peptide technology
(i) peptide radiopharmaceuticals as neurodiagnostic agents –all human malignant gilomas overexpress the gene encoding for the epidermal growth factor(EGF) receptor (EGF-R). Owing to the selective overexpression of the EGF-R in many human brain gilomas. It is possible that EGF could be used as a peptide radiopharmaceutical for the early diagnosis of brain cancer.
(ii) Neurotrophin neuroprotection in stroke – small molecules neuroprotective either do not cross the BBB or have high toxicity profiles that preclude their clinical use . in contrast , the safety profiles of large molecules neurotrophin neurotherapeutics, , such as brain – derived neurotrophins factor (BDNF) would be expected to be more favorable however large molecules neurotrophins such as BDNF don’t cross the BBB.
4.Non-viral gene therapy of the brain –Brain targeting via gene therapy employ either cationic liposomes or viral vectors and neither of these cross the BBB . This necessitates the use of intracerebral injection of gene and this allows for an able to have widespread expression of an exogenous gene throughout the brain and the only way this can achieved is by delivering the exogenous gene through the walls of the capillaries that perfuse the brain . In the human brain , the total length of capillaries is about 400 miles so a drug or gene will instantaneously distribute throughout the CNS once the BBB is traversed1,6.
REFERENCES
1. Mazza M, Uchegbu LF, Schatzlein AG, et al. cancer and blood brain barrier Trojan horses for courses 2008 Sep;155(2);149-151.
2. Pardridge WM, Brain drug targeting and gene technologies .2001 April 4;87,97-103
3. Jain NK. Progress in controlled and novel drug delivery system .first edition ,2004: 23.
4. Wilson. Brain targeting pbca nanoparticle and the blood brain barrier 2009;4(5):499-502.
5. Allen LV, Nicholas J, Ansel C. Pharmaceutical dosage form and drug delivery system. Eight edition, 652
6. Pardridge WM, Blood brain barrier drug targeting the future of brain drug development 2003 March; 91-101.
7. Misra A, Ganesh S, Shahiwala A, et al. Drug delivery to the central nervous system. 2003 Aug;6 (2) :252-273
8. Vyas TK, Babbar AK,Sharma RK, et al, A preliminary brain targeting studies on intranasal mucoadhesive microemulsion of sumatriptan .2006;6(4).
9. Orive G, Hernandez RM, Gascon AR, et al. Micro and nano drug delivery system in cancer therapy 2005 March ; 131-138.
10. Singer E, Targeting the brain with sound wave, non invasive way to control brain activity 2009 June :1-2
11. Jaypraka M, Ramnar J, Shah S,et al. Overview of brain targeting drug delivery system, 2009 .
12. Soni V, Chourasia MK, Gupta Y, et al. Novel approches for drug delivery to the brain. 2004 June;66(6):711-720.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






