

ABOUT AUTHORS:
Dhakar K Mukesh*, Dashora Ahok, Kumar Neeraj
Geetanjali Institute of Pharmacy,
Udaipur
*dhakarmukesh03@yahoo.com
ABSTRACT:
Alien hand syndrome was first identified in 1908, it was not clearly defined until 1972. Depending on the cause of the injury, the movements may be random or purposeful, and may affect the dominant or non-dominant hand. Alien hand syndrome (anarchic hand or Dr. Strangelove syndrome) is an unusual neurological disorder in which one of the sufferer's hands seems to take on a mind of its own. An individual with this neurological disorder has full sensation in the rogue hand, but is unable to control its movements, and does not feel that it is a part of their body. The symptoms are brought on by an injury to the brain, such as head trauma, stroke, tumor, or infection, but it can also be a side effect of a certain kind of brain surgery. As a side effect of brain surgery, or an injury to the corpus callosum (the area of the brain which connects the two halves of the brain). known treatment for Alien Hand Syndrome at this time though the symptoms can be reduced by keeping the alien hand occupied and involved in a task.
Reference ID: PHARMATUTOR-ART-1952
INTRODUCTION:
Alien hand syndrome (anarchic hand or Dr. Strangelove syndrome) is an unusual neurological disorder in which one of the sufferer's hands seems to take on a mind of its own. AHS is best documented in cases where a person has had the two hemispheres of their brain surgically separated, a procedure sometimes used to relieve the symptoms of extreme cases of epilepsy. It also occurs in some cases after other brain surgery, strokes, or infection. There is a very real, very disturbing, and very rare medical condition called “Alien Hand Syndrome” (AHS). An individual with this neurological disorder has full sensation in the rogue hand, but is unable to control its movements, and does not feel that it is a part of their body. The hand becomes personified, as if it has a will of its own, and its owner will usually deny ownership of the limb.
Clinical Aspects of Alien Hand Syndrome :
AHS is a rare neurological disorder characterized by a loss of the sense of agency associated with the purposeful movement of the limb while retaining a sense of ownership. The patient has no control over the movements, instead, the hand has the capability of acting autonomously, independent of their voluntary control. The affected hand can perform complex acts. In one of the first clinical papers, the authors coined the term “main estranger” when describing the puzzling behaviour of some patients who failed to recognize their own left hand when deprived of visual feedback after callosotomy.This complex phenomenon may present in different variants which are caused by different lesions. According to Brian and Chattered , the phenomenon of AHS can be categorized as:- a) coordinative disturbances in bimanual behaviour caused by conflicts arising while using both hands (e.g. intermanual conflict [hands acting at cross-purposes to each other], diagnostic behaviour [conflict between desired and performed act] or agonistic apraxia [automatic execution of orders by one hand while using the other hand]), b) purposefulness of movements (e.g. compulsive manipulation of tools [manipulating objects by the abnormal hand against their own will, sometimes referred to as “anarchic hand” autonomous behaviour of the hand without the denial of ownership, or magnetic/repellent apraxia [instinctive grasping/ avoidance hand movements] c) subjective reactions of the affected subject toward this limb (e.g. interhemispheric autocriticism [overt astonishment caused by the behaviour of the abnormal hand], or stranger’s hand sign [denial of ownership of the hand]). The patient is conscious of the deficit and usually the deficit is not associated with apraxia. The deficit can fluctuate and often depends on attentional and emotional status of the patient. There is a tendency of perseveration and often the movements are driven by objects in the peripersonal space of the patients. Many patients h t.ave an inter manual conflict.
a) coordinative disturbances in bimanual behaviour caused by conflicts arising while using both hands (e.g. intermanual conflict [hands acting at cross-purposes to each other], diagnostic behaviour [conflict between desired and performed act] or agonistic apraxia [automatic execution of orders by one hand while using the other hand]), b) purposefulness of movements (e.g. compulsive manipulation of tools [manipulating objects by the abnormal hand against their own will, sometimes referred to as “anarchic hand” autonomous behaviour of the hand without the denial of ownership, or magnetic/repellent apraxia [instinctive grasping / avoidance hand movements] c) subjective reactions of the affected subject toward this limb (e.g. interhemispheric autocriticism [overt astonishment caused by the behaviour of the abnormal hand], or stranger’s hand sign [denial of ownership of the hand]). The patient is conscious of the deficit and usually the deficit is not associated with apraxia. The deficit can fluctuate and often depends on attentional and emotional status of the patient. There is a tendency of perseveration and often the movements are driven by objects in the peripersonal space of the patients. Many patients h t.ave an inter manual conflict.
ALIEN HAND SYNDROME – SUBTYPES:
There are several distinct subtypes of Alien Hand that appear to be associated with specific types of triggering brain injury. Damage to the corpus callosum can give rise to "purposeful" actions in the sufferer's non-dominant hand (a right-handed sufferer's left hand will turn alien, and the right hand will turn alien in the left-handed) as well as a problem termed "intermanual conflict" in which the two hands appear to be directed at opposing purposes, whereas unilateral injury to the brain's frontal lobe can trigger reaching, grasping and other purposeful movements in the contralateral hand. With frontal lobe injury, these movements are often exploratory reaching movements in which external objects are frequently grasped and utilized functionally, without the simultaneous perception on the part of the patient that they are "in control" of these movements.
ALIEN HAND SYNDROME – SYMPTOM:
The list of signs and symptoms mentioned in various sources for Alien hand syndrome includes the 3 symptoms listed below:
1. Lack of awareness of arm movement or actions
2. Lack of control over arm movement
3. Inability to feel control over hands movements.
ALIEN HAND SYNDROME – CAUSES:
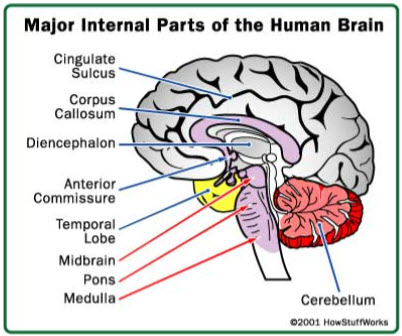
Fig.: Damage to the corpus collosum is at the heart of this rare disorder.
There are several distinct subtypes of Alien Hand that appear to be associated with specific types of triggering brain injury. Damage to the corpus callosum can give rise to "purposeful" actions in the sufferer's non-dominant hand (a right-handed sufferer's left hand will turn alien, and the right hand will turn alien in the left-handed) as well as a problem termed "intermanual conflict" in which the two hands appear to be directed at opposing purposes, whereas unilateral injury to the brain's frontal lobe can trigger reaching, grasping and other purposeful movements in the contralateral hand. With frontal lobe injury, these movements are often exploratory reaching movements in which external objects are frequently grasped and utilized functionally, without the simultaneous perception on the part of the patient that they are "in control" of these movements.
ALIEN HAND SYNDROME- TREATMENT :
There is no known treatment for Alien Hand Syndrome at this time though the symptoms can be reduced by keeping the alien hand occupied and involved in a task. Proposed Strategies For Treatment:
Clonazepam
Not to be confused with camazepam, chlorpromazine, cinolazepam, or clobazam. Clonazepam
Systematic (IUPAC) name
5-(2-chlorophenyl)-7-nitro-2,3-dihydro-1,4-benzodiazepin-2-one
Clonazepam is a benzodiazepine drug having anxiolytic, anticonvulsant, muscle relaxant, and hypnotic properties. It is marketed by Roche under the trade name Klonopin in the United States and Rivotril in Australia, Brazil, Canada and Europe (and in countries like Serbia, Macedonia, Croatia and Montenegro). Other names such as Ravotril, Rivatril, Clonex, Paxam, or Kriadex are known throughout the rest of the world.[citation needed] Clonazepam has an unusually long half-life of 18–50 hours, making it generally considered to be among the long-acting benzodiazepines. Clonazepam is a chlorinated derivative of nitrazepam and therefore a chloro-nitrobenzodiazepine.
Pharmacology of Clonazepam
Clonazepam's primary mechanism of action is via modulating GABA function in the brain, via the benzodiazepine receptor, located on GABAA receptors, which, in turn, leads to enhanced GABAergic inhibition of neuronal firing. Benzodiazepines do not replace GABA but rather enhance the effect of GABA at the GABAA receptor by increasing the opening frequency of chloride ion channels which leads to increased inhibitory effects with resultant central nervous system depression. In addition clonazepam decreases the utilization of 5-HT (serotonin) by neurons and has been shown to bind tightly to central type benzodiazepine receptors. Because clonazepam is effective in low milligram doses (0.5 mg clonazepam = 10 mg diazepam), it is said to be among the class of "highly potent" benzodiazepines. The anticonvulsant properties of benzodiazepines are due to enhancement of synaptic GABA responses and inhibition of sustained high frequency repetitive firing.
Benzodiazepines acted via micromolar benzodiazepine binding sites as Ca2+ channel blockers and significantly inhibit depolarization-sensitive calcium uptake in experimentation on rat brain cell components. This has been conjectured as a mechanism for high-dose effects on seizures in the study.
REVIEW OF LITERATURE:
1.J Marey-Lopez, E Rubio, et al Neurosurg Psychiatry 2002;73:447–449.
The alien hand syndrome, as originally defined, should be reserved for cases in which the hand feels foreign “together with” observable involuntary motor activity. These involuntary movements are unusual during or after acute stroke. Three varieties of alien hand syndrome have been reported, involving lesions of the corpus callosum alone, the corpus callosum plus dominant medial frontal cortex, and posterior cortical and subcortical areas. A patient with posterior alien hand syndrome of vascular aetiology is reported. Imaging studies disclosed an isolated infarction of the right thalamus sparing other cerebral regions.
The patient received antiaggregant treatment with ticlopidine. Initial brain computed tomography performed at admission showed a right thalamic infarct. Follow up magnetic resonance imaging three days after onset revealed T1(TR 700 ms, TE 20 ms) and T2 (TR 2700 ms, TE 95 ms) weighted images, an infarct in the ventral posterolateral and dorsal portion of the right thalamussparing the posterior limb of the internal capsule and the mesencephalon. No lesions were detected in the corpus callosum or other cerebral regions .
2.The Alien Hand: Cases, Categorizations, and Anatomical Correlates
Lisa A. Scepkowski , Alice Cronin-Golomb Boston University
The clinical characteristics and neuroanatomical damage reported in more than 50 published cases of observed “alienhand” signs are reviewed. The terms alien-hand sign and alien-hand syndrome describe phenomena experienced by patientsin which an upper limb performs complex motor activities outside of volitional control. The categories of frontal and callosal subtypes and their relation to behavior and neuropathology are evaluated with reference to the dual premotor system theory, which emphasizes the role of the supplementary motor areas in alien-hand phenomena. Detailed consideration is given to the more recently described posterior subtype, which is purported to result from damage to the parietal lobe or other posterior brain areas. The lack of uniformity in reported assessment methods (behavioral tests, neuroimaging) in published cases contributes to the difficulty in establishing clear subtypes of alien-hand phenomena. Suggestions are made regarding current categorizationsand available assessment methods.
3.(J Neurol Neurosurg Psychiatry 1995;58:735-737)
A 58 year old right handed woman developed a left alien hand syndrome after a right capsulothalamic haemorrhage with mesencephalic extension. No lesion was detected in the corpus callosum. Positron emission tomography suggested that right cortical dysfunction might account for the absence of recognition of the left hand whereas involuntary motor activity was attributed to the lesion itself. This case shows that the alien hand syndrome is not always the expression of a disconnection syndrome and may occur after a large, strategically located, posterior lesion.
The alien hand syndrome was recently defined as a strange or foreign feeling of one's hand, failure to recognise its ownership without visual cue, together with observable involuntary motor activity.' Originally Brion and Jedynak2 described the alien hand syndrome in four patients with corpus callosum tumours. Since then all reported cases of alien hand syndrome have had, to our knowledge, some kind of corpus callosum esion. 4 5We describe a patient with the alien hand syndrome attributed to a unique lesion sparing the corpus callosum, and attempt to explain the symptomatology by anatomoclinical correlations with radiological findings and metabolic information provided by PET 4.(7 Neurol Neurosurg Psychiatty 1993;56:788-792).
4. Doody RS, Jankovic J. The alien hand and related signs. J Neurol Neurosurg Psychiatry 1992;55:806–810.
one's limb when visual cues are removed, a feeling that one body part is foreign, personification of the affected body part, or autonomous activity which is perceived as outside voluntary control.1 Although the hand is most frequently affected, any limb or Alien hand syndrome (AHS) or alien limb sign includes failure to recognize ownership of combination of limbs may fulfill the alien limb criteria.
Two types of AHS have been described. Frontal AHS occurs in the dominant hand and is associated with reflexive grasping, groping, and compulsive manipulation of tools. It is a result of damage to the supplementary motor area, anterior cingulate gyrus, and medial prefrontal cortex of the dominant hemisphere and anterior corpus callosum. Callosal AHS is characterized by intermanual conflict and requires only an anterior callosal lesion. Callosal AHS is best explained by hemispheric disconnection manifested during behaviors requiring dominant hemisphere control.
We hypothesize that the alien limb symptoms that our patient demonstrated were secondary to the lesion in the anterior corpus callosum; however, some of his behavioral manifestations may have been exacerbated by the concurrent right parietal stroke. The latter may be associated with hemispa-tial neglect, typically characterized by directional hypokinesia for actions into and toward contralesional hemispace or failure to respond to stimuli on the left side.3 Anosognosia, or unawareness of the neurologic deficit, is frequent after right parietal lesions, and may compound the disability deriving from the neglect itself,3,4 although no characteristic features of neglect were observed in our patient
Table 1.
Terms and clinical signs in Alien Hand Syndrome :-
|
Term |
Definition |
|
Alien hand syndrome / Alien hand sign |
Alien hand syndrome / Alien hand sign |
|
Posterior alien hand |
The alien hand syndrome that may follow posterior lesions, characterized by hand levitation and abnormal postures. |
|
Type of aberrant motor behaviour of the alien hand |
|
|
Magnetic apraxia / repellent apraxia |
Instinctive grasping/avoiding with an abnormal posture. |
|
Compulsive manipulation of tools |
Manipulating objects by the abnormal hand against the patient’s own will. This term is used mainly in the Japanese literature. |
|
Anarchic hand |
Autonomous behavior of a limb without the denial of ownership |
|
Subjective |
|
|
Stranger’s hand sign |
Denial of ownership of a limb. |
|
Strange hand sign |
The original meaning of the alien hand sign (la main étrangère). Failure to recognize the abnormal hand as one’s own hand. |
|
Autocriticism, interhemispheric autocriticism |
Expression of astonishment with the behaviour of the abnormal hand. |
|
Interhand interaction |
|
|
Diagonistic dyspraxia |
A conflict between the desired act and the performed act. |
|
Intermanual conflict |
The hands act at cross-purposes to each other. |
|
Agonistic dyspraxia |
Compulsive automatic execution of orders by one of the hands when the patient is asked to perform the movement with the other hand |
Summary:
Alien hand syndrome (AHS) is a neurological disorder in which movements are performed without awareness or conscious will. Phenomena like awareness or consciousness are still poorly studied in physiology and have only become a crucial topic in neuroscience in the last few years. Pertinent experiments in which the volitional control of a movement was studied unanimously, demonstrate that movements are initiated before consciousness occurs. By doing so, the brain adopts internal anticipatory models of voluntary action. Several studies suggest that the parietal cortex is important in activating and maintaining such internal models of action. AHS is characterized by a loss of the sense of agency associated with the purposeful movement of the limb while retaining a sense of ownership. The hand seems toper form acts without intentional guidance by the patient. Thus, the patient has no control over the movements; instead, the hand has the capability of acting autonomously, independent of patient’s voluntary control. This complex phenomenon may present in different variants which are caused by different lesions and can be categorized by several dimensions:
- type of aberrant behavior performed by the affected hand;
- coordinative disturbances in a bimanual behavior, caused by conflicts arising while using both hands;
subjective reactions of the affected individual toward this limb. The syndrome and its variants is caused by lesions to the medial frontal lobe, the corpus callosum and the parietal areas, but can also appear within neurodegenerative diseases, such as corticobasal degeneration, and may even precede them (e.g. Creutzfeldt-Jakob disease). In a functional MRI study of AHS, major activation was reported for the frontal inferior gyrus of the dominant hemisphere in voluntary movement of the affected hand, suggesting an important role of this area in organizing willed actions. Neuropsychological investigations indicate an involvement of a supramodal attentional system in the organization of movements. AHS serves as a paradigm to study the conscious experience of movement and can be considered as a neurological disorder of will. This review discusses some physiological as well as functional-neuroanatomical aspects, by reporting some actual studies relating AHS to consciousness and will.
BIBLIOGRAPHY
1.Akelaitis AJ (1945) Studies of the corpus callosum. IV. Diagonistic dyspraxia in epileptics following partial and complete section of the corpus callosum. Amer J Psychiatr 101: 594-599.
2.Akelaitis AJ, Risteen W, Herren R, Van Wagenen W (1942) Studies of the corpus callosum. III. A contribution to the study of dyspraxia and apraxia following partial and complete section of the corpus callosum. Arch Neurol Pyschiatr 47: 971-1008. 1972;126:257-66.
3.Andersen RA, Buneo CA. Intentional maps in posterior parietal cortex. Ann Rev Neurosci. 2002;25:189–220.
4.Bogen J (1979) The callosal syndromes: In: Heiman K, Valenstein E (eds). ClinicalNeuropsychology. Oxford University Press Oxford, pp 337-407.
5.Brion S, Jedynak CP (1972) Troubles du transfert interhémispherique (callosal disconnection) a propos de trois observations de tumeurs du corps calleux. Le signe de la main étrangère. Rev Neurol 126: 257-266.
6.Bogen JE. The callosal syndromes. In: Heilman KM, Valenstein E, eds. Clinical Neuropsychology. 2nd ed. New York: Oxford University Press, 1985:295-338.
7.Brion S, Jedynak CP. Troubles du transfert interhemispherique.A propos de trois observations de tumeurs du corps calleux. Le signe de la main etrangere. Rev Neurol
8.Buxbaum LJ, Ferraro MK, Veramonti T, et al. Hemispatial neglect: subtypes, neuroanatomy, and disability. Neurology 2004;62:749–756. Abstract/FREE Full Text
9.Della Sala S, Marchetti C, Spinnler H (1991) Right-sided anarchic (alien) hand: a longitudinal study. Neuropsychologia 29: 1112-1117.
10.Della Sala S, Marchetti C, Spinnler H (1994) The anarchic hand: a fronto-mesial sign.In: Boller G, Grafman J (eds) Handbook of Neuropsychology. Vol. 9. Elsevier Amsterdam pp 233-255.
11.Della Sala S, Marchetti C, Spinnler H (1994) The anarchic hand: a fronto-mesial sign.
12.Eidelberg D, Dhawan V, Moeller JR, et al. The metabolic landscape of cortico-basal ganglionic degeneration: regional asymmetries studied with positron emission tomography. Jf Neurol Neurosurg Psychiatry 1991;54: 856-62.
13.Fisher CM (2000) Alien hand phenomena: a review with the addition of six personal cases. Can J Neurol Sci 27:183-190.
14.Foix C, Hillemand P. Les syndr6mes de la region thalamique.La Presse Midicale 1925;8:113-7.
15.Feinberg TE, Schindler RJ, Gilson Flanagan N, Haber LD. Two alien hand syndromes. Neurology 1992; 42:19-24.
16.Feinberg TE, Schindler RJ, Flanagan NG, Haber LD. Two alien hand syndromes. Neurology 1992;42:19–24. Abstract/FREE Full Text
17.Goldberg G (1987) From intent to action: evolution and function of the premotor systems in the frontal lobe. In: Perecman E (ed) The Frontal Lobes Revisited. I.R.B.N. Press New York, pp 273-306.
18.Goldberg G, Mayer N, Toglia J (1981) Medial frontal cortex infarction and the alien hand sign. Arch Neurol 38: 683-686.
19.Gibb WRG, Luthert PJ, Marsden CD. Corticobasal degeneration. Brain 989;112:1171-92.
20.Hallett M. Volitional control of movement: the phisiology of free well. Clinical Neurophisiology. 2007;118 (6):1179–92.
21.Inzelberg R, Nisipeanu P, Blumen SC, Carasso RL (2000) Alien hand sign in Creutzfeldt-Jacob disease. J Neurol Neurosurg Psychiatr 68: 103-104.
22.Libet B, Gleason CA, Wright EW, Pearl DK. Time of conscious intention to act in relation to onset of cerebral activity (readiness potential). The unconscious initiation of a freely voluntary act. Brain. 1983;106:623–42.
23.Levine DN, Calvanio R, Rinn WE. The pathogenesis of anosognosia for hemiplegia. Neurology 1991;41:1770–1781. Abstract/FREE Full Text
24.Levine DN, Rinn WE. Opticosensory ataxia and alien hand syndrome after posterior cerebral artery territory infarction. Neurology 1986;36:1094-7.
25.Leiguarda R, Starkstein S, Nogues M, Berthier M, et al. Paroxysmal alien hand syndrome. Jf Neurol Neurosurg Psychiatry 1993;56:788-92.
26.Milandre L, Brosset C, Gabriel B, Khalil R. Mouvementsinvolontaires transitoires et infarctus thalamiques. Rev Neurol 1993;149:402-6.
27.Porro AC. (1996). Primary motor and sensory cortex activation duringmotor performance and motor imagery: a functional magnetic resonanceimaging study. J Neurosci 1996;16:7688–98.
28.Sacco L, Calabrese P. Alien hand syndrome: a neurological disorder of will. Schweiz Arch Neurol Psychiatr. 2010;161(2):60–3.
29.Searle JR. How to study counsciousness scientifically. Biol Sci. 1998;353(1377):1935–42.
30.Smith Doody R, Jankovic J. The alien hand and related signs. J Neurol Neurosurg Psychiatry 1992;55:806-10.
31.Tanaka Y, Iwasa H, Yoshida M. Diagnostic dyspraxia: case report and movement-related potentials. Neurology 1990;40:657-61.
32.Vanek ZF, Jankovic J (2000) Dystonia in corticobasal degeneration. Adv Neurol 82: 61-67.
33. jnnp.bmj.com/content/58/6/735#related-urls
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






