

 About Authors:
About Authors:
Gupta S*, Singal A
Apex Institute Of Pharmaceutical Sciences,
Jaipur, Raj., India
*somesh.gupta88@gmail.com
Abstract
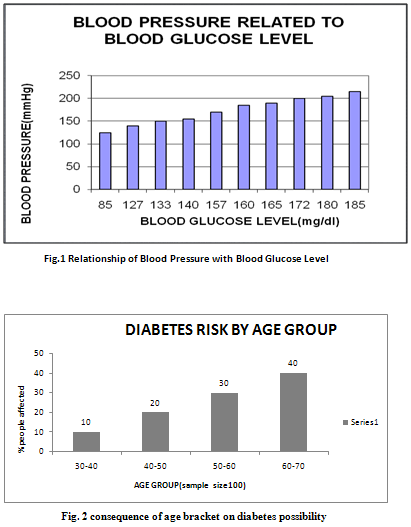
The aim of the present study was to correlate the occurrence of hypertension in the diabetics’ patient by the survey report on hypertension associated with diabetics’ patient. The effect of this study is symbolize that 70% patient have diabetes with hypertension and 30% patient with hypertension only so we can say that in this survey as the BGL increased leads to increased in B.P. And it was also found to be that aged patients have more risk of diabetes. Over 60- 70 year age group patient have 40% risk to get diabetes.
[adsense:336x280:8701650588]
Reference Id: PHARMATUTOR-ART-1384
INTRODUCTION:-
Hypertension: - It can define as the condition where blood pressure is elevated to an extent where Clinical benefit is obtained from blood pressure lowering.1
Diabetes Mellitus: - Diabetes mellitus (DM) is the name given to a group of disorders characterized by chronic hyperglycemia, polyurea, polydipsia, polyphagia, emaciation and weakness, in which the sugar level is above the normal sugar level 80-120 mg/dl of the whole blood.2
Hypertension Associated With Diabetes:-
The Coexistence of Type 2 Diabetes and Hypertension:-Coexistence may lead to-
1. Doubling of cardiovascular events
2. Abnormalities in central & peripheral parameters of cardiovascular structure and function
That precedes the clinical manifestation of cardiovascular disease.
a. Increased left ventricular mass and wall thickness.
b. Left ventricular diastolic filling abnormalities
c. Impaired endothelial function Such as-
* Impairments of the Nitric oxide (NO) pathway
* Production of cyclooxygenase-dependent vasoconstrictor
* Enhanced production of oxidative stress
* Increased arterial stiffness and systemic inflammation3,4,5
Symptoms: - Dyspnoea, Chest-pain, Blurred-vision, Slight edema, Constipation, Tiredness6, 7
[adsense:468x15:2204050025]
Complication of Hypertension in Diabetes Mellitus:-
Micro vascular Complications: - Renal disease, Sexual dysfunction, Orthostatic hypotension, Eye disease
Macro vascular complications: - Cerebrovascular disease, Cardiac disease, Peripheral vascular disease1, 8, 9
Prevalence:-
* The prevalence of hypertension in the diabetic population is 1.5-3 times higher than that of nondiabetic age-matched groups.
* The timing and presentation of hypertension differs between type 1 and type 2 diabetes.
* In type 1 diabetes, hypertension develops after several years of the disease and usually reflects the development of diabetic nephropathy. It ultimately affects ~30% of individuals with type 1 diabetes.
* In type 2 diabetes, hypertension may be present at the time of diagnosis or even before the development of hyperglycemia.10,11
Pathophysiology: -
In the presence of nephropathy, extracellular fluid volume and total body sodium levels are increased. The activity of the renin-angiotensin-aldosterone system (RAAS) is reduced in these patients. Studies in humans with hypertension have found hyperinsulinemia secondary to insulin resistance and decreased insulin clearance. Hyperinsulinemia may possibly be associated with increased renal sodium resorption and sympathetic nervous system over activity, leading to hypertension in obese individuals and other insulin-resistant states, such as type 2 diabetes.12
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Review of Pharmacological Agent in MOHID:-
Step-1 LifestyleModification:-
* Regular aerobic physical activity
* Reduction of sodium intake
* Smoking cessation
* Dietary intervention to control hyperglycemia and dyslipidemia
* Weight reduction
* Moderation of alcohol intake(Take Step-2 if Inadequate Response (after 3 months))
Step-2 Continue Lifestyle Modification plus…………
Initiate pharmacologic selection (in alphabetical order)
* ACE inhibitor
* Alpha-receptor blockers
* Calcium antagonist
* Other diuretics(in low dose are preferred bcz of fewer adverse effects On glucose homeostasis, lipid profile and renal function)
* (ACE inhibitor are drugs of choice in patient with albuminuria/proteinuria)
* (Beta-blockers can adversely affects peripheral blood flow, prolong hypoglycemia and mask hypoglycemia symptoms) (Take Step-3 if Inadequate Response)
Step-3 Increase drug dose or Substitute another drug or Add a second agent from a different class (e.g. diuretics, if not selected).4
METHOD: -
Number of patient -
100 patient were considered for this survey report
Material-
To measure the blood glucose level (BGL) I have used glucometer (Company-Tanayil FZE) and for blood pressure (B.P) I have used sphygmomanometer (Company-Apothecaries fundries Mfg Corporation New Delhi, India)
Parameter (In-Vivo) –
Two parameter i.e. Blood glucose level (fasting P.P.2hr) and Blood pressure was measured for the preparation of survey report. Study (survey) was done on 100 patients. For the completion of this task I did contact to various hospitals (S.M.S, Escort Fortis, Tagore, sanjeevani, sakat, and tongia) and laboratories. Where I was selected patient those having hypertension or diabetes or both and concerned about their life style, regular medicines and observed various parameters (BGL level, B.P, lipid profile, blood urea etc.). B.P measured by using well mainted sphygmomanometer of validated accuracy. B.P measured in both arms and the arm with the highest value used for subsequent reading. Patient with diabetes having nephropathy in which glomerular filtration rate (GFR) is increased. This can be estimated by using serum creatinine.high concentration of glucose in blood is converted into cholesterol and deposited inner side of artery. This leads to increased thickness of wall of artery and generate pressure. So concluded that patient with diabetes have more risk of hypertension compared with non-diabetics patient.
RESULTS:-
The results of the studies support an aggressive approach to the diagnosis and treatment of hypertension in patients with diabetes in order to substantially reduce the incidence of both macro vascular and micro vascular complications.
By the patient survey report finally we concluded that 70% diabetic patient have hypertension also. Only 30% patient suffered with hypertension only. And it was also found to be that aged patients have more risk of diabetes. Over 60- 70 year age group patient have 40% risk to get diabetes.
Hypertension occurs with twice the frequency in the diabetic in compared with the non-diabetic population
CONCLUSION:-
Hypertension is associated with diabetes. Largely independent of age and obesity. Although abdominal visceral obesity is an especially strong risk factor for the development of both conditions. Hypertension is part of the metabolic syndrome. With a prevalence as high as 60% in patients who have type 2 diabetes The effect of this study is symbolize that 70% patient have diabetes with hypertension both because they have blood glucose level more than and equal to 140mg/dl and 30% patient with hypertension only because they have BGL <140mg/dl, so we can say that in this survey as the BGL increased leads to increased in B.P. And it was also found to be that aged patients have more risk of diabetes. Over 60- 70 year age group patient have 40% risk to get diabetes.
ACKNOWLEDGEMENT:-
Author would like to give thanks to Dr. Sachin Jawar (Apex hospital) and Asst. Prof. Anil Singal (MGRP, University)
REFERENCES:-
1. Walker Roger, Whittlesea Cate, Clinical Pharmacy and therapeutics, Fourth Edition, Churchill Livingstone Page no: 265-79,629-55.
2. Deb L, Dutta A, Diabetes mellitus its possible pharmacological evaluation techniques and naturotherapy, International Journal of Green Pharmacy, 1, 2006, Page no: 15-28.
3. Kerry J. Stewart, EdD, FAACVPR, FACSM, FSGC, Role of Exercise Training on Cardiovascular disease in persons who have type 2 diabetes and hypertension, Journal of diabetes and cardiovascular disease: cardiology clinics, Nov 2004, Vol-22, Page no:569-70,77.
4. Cristina B. Guzman and James R. Sowers, Special Considerations in the therapy of Diabetic Hypertension, Journal of Progress in Cardiovascular disease, July/Aug 1998, Vol-41, Page no: 461-62,68.
5. Nasser Mikhail, Michael S. Golub, and Michael L. Tuck, Obesity and Hypertension, Journal of Progress in Cardiovascular disease, July/Aug 1999, Vol-42, Page no:39-49.
6. Anonymous: NEWSPAPER-TIMES OF INDIA, Accessed on 14 Nov 09.
7. Anonymous: en.wikipedia.org/wiki/Hypertension, Accessed on 5 Nov 2009.
8. Ghosh MN, Fundamentals of Experimental Pharmacology, 3rd edition, 2005, Hilton and Company, 190-197.
9. Bertram G. KATZUNG, Basic and clinical Pharmacology, Mc Graw Hill LANGE, 10TH edition, Page no: 587-92.
10. Harris MI, Flegal KM, Cowie CC, Eberhardt MS, Goldstein DE, Little RR, et al. Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988-1994. Diabetes Care 1998;21:518-24
11. The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med 1997;157:2413- 46
12. Errol D, Crook M D, Associate Professor and acting chair, department of Internal Medicine Wayne state University School of Medicine staff Physician, John D. Dingell VAMC
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






