

 About Authors:
About Authors:
S Hamza*1, Dr Tanveer Aalam2, Dr Asma3
1* Assistant Professor, Department of Pharmacology,
Shree M V Shah Pharmacy college,
Gajan, Modasa: 383315, Gujarat.
2 Department of Emergency Medicine,
Apollo hospitals International Ltd,
Bhat GIDC estate, Gandhinagar: 382428, Gujarat.
3 Medical Officer, Civil Hospital,
Ahmadabad: 380 002. Gujarat, India
ABSTRACT:
India suffers from the highest number of deaths - around 1,05,000 in absolute terms annually- due to road accidents in the world owing to poor infrastructure and dangerous driving habits according to the World Health Organisation1. Calling road fatalities an "epidemic" that will become the world's fifth biggest killer by 20302. It is said that 90% of deaths on the world's roads occur in low and middle-income countries (21.5 and 19.5 per lakh of population, respectively) though they have just 48% of all registered vehicles.
[adsense:336x280:8701650588]
The statistics for India are chilling. At least 13 people die every hour in road accidents in the country, the latest report of the National Crime Records Bureau reveals3. In 2007, 1.14 lakh people in India lost their lives in road mishaps — that’s significantly higher than the 2006 road death figures in China, 89,455.
Many studies involving victims of road traffic accidents which were conducted in India have highlighted the fact that majority of the victims of trauma were transported to the first hospital either by auto rickshaw or private 4 wheelers with absolutely no first aid. And among those who were transported by ambulances, none of them received treatment which would have benefited them in any way. Nonexistent prehospital care4
Emergency medicine is a medical specialty—a field of practice based on the knowledge and skills required for the prevention, diagnosis and management of acute and urgent aspects of illness and injury affecting patients of all age groups with a full spectrum of undifferentiated physical and behavioral disorders. It further encompasses an understanding of the development of pre-hospital and in-hospital emergency medical systems and the skills necessary for this development.
Lack of emergency care is a massive problem in countries whose health systems are too weak to provide this crucial part of health care, resulting in many preventable deaths—rather more important than the preventable hospital admissions cited as a huge problem in the English report5- ‘Trends in emergency admissions in England 2004 – 2009: is greater efficiency breeding inefficiency?. So, it seems today a great necessity to understand the importance of EM (Emergency Medicine) and creating its awareness.
REFERENCE ID: PHARMATUTOR-ART-1255
[adsense:468x15:2204050025]
IMPORTANT IN THIS ARTICLE:
INTRODUCTION:
Expansion in road network, motorization and urbanization in the country has been accompanied by a rise in road accidents leading to road traffic injuries (RTIs) and fatalities as a major public health concern. Today road traffic injuries are one of the leading causes of deaths, disabilities and hospitalizations with severe socioeconomic costs across the world. Despite strong laws and regulations, India has been unable to prevent the growing number of accidents on its roads. With around 1,05,000 death deaths annually, the country has overtaken China6.
As per the Commission for Global Road Safety (2009), road traffic accidents kill an estimated 1.3 million people and injure 50 million people per year globally, and global road fatalities are forecast to reach 1.9 million by 20207. It is estimated that the number of deaths from road accidents in Asia is about 700,000 per year, accounting for more than half of the world’s road fatalities even though Asia accounted for only 43% of the global vehicle population in 20078.
During the year 2009 there were around 4.9 lakh road accidents which killed 1,25,660 people and injured more than 5 lakh persons in India. These numbers translate into one road accident every minute and one road accident death every four minutes for India. Road traffic injuries and fatalities impose a huge economic burden on developing economies in particular. In India more than half of the road accident victims are in the age group (25-65 years), the key wage earning and child raising age group. The loss of the main bread earner and head of household due to death or disability can be catastrophic, leading to lower living standards and poverty, in addition to the human cost of bereavement.
In the year 2004, the National Human Rights Commission constituted an Expert Group to study the existing system for emergency medical care in India to suggest appropriate methods of emergency medical care, which should be developed by different States/Union-Territories and their essential components.
The expert group submitted a Report on 7th April 2004. It reviewed the existing scenario and the Centralized Accident and Trauma Services (ATS) and stated that nearly 4 lakh persons lose their lives annually due to injuries, nearly 75 lakh persons are hospitalized and three and half lakh persons who receive minor injuries get emergency care at various places in India9. However, present Emergency Medical Support (EMS) in the country is functioning sub-optimally and requires upgradation. The Report revealed the lacunae, which exist in the present EMS and made a number of recommendations for implementation in the short term and in the long-run. These recommendations were sent to the Health Services and the States and UTs.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
PROFILE OF ACCIDENTAL CAUSALITIES:
World scenario:
Using published data as a base, the study estimates that in 1999 between 750,000 and 880,000 people may have died as a result of road accidents and that the majority of these deaths occurred in developing and emerging nations, with approximately half in the Asia-Pacific region alone. Road fatalities are expected to continue to increase with a fatality toll estimated between 900 thousand and 1.1 million by the year 2010 and between 1.1 and 1.3 million by 202010.
Results also show that the highest fatality rates (deaths per 10,000 motor vehicles) worldwide occur in African countries, particularly Ethiopia, Uganda and Malawi whilst fatality risk (deaths per 100,000 populations) is highest in a disparate group of countries including Thailand, Malaysia, South Africa and Saudi Arabia11.
Table No: 01: Motor vehicle deaths (most recent) by country
|
RANK |
COUNTRIES |
DEATH RATIO |
|
0 |
United states |
15.5 deaths per 100,000 people |
|
02 |
Belgium |
15.4 deaths per 100,000 people |
|
03 |
New Zealand |
14 deaths per 100,000 people |
|
04 |
France |
13.7 deaths per 100,000 people |
|
05 |
Italy |
12.9 deaths per 100,000 people |
|
06 |
Ireland |
11.6 deaths per 100,000 people |
|
07 |
Austria |
10.4 deaths per 100,000 people |
|
08 |
Australia |
10 deaths per 100,000 people |
|
09 |
Germany |
9.8 deaths per 100,000 people |
|
10 |
Canada |
9.6 deaths per 100,000 people |
In USA, death due to road accidents is the leading cause of mortality amongst the five main causes including suicide, cancer and heart disease12.
Table: 01: Five Leading Causes of Death, USA, Ages 15-24, 1998
|
CAUSE |
PERCENT OF TOP 5 |
NUMBERS |
|
(1) Accidents |
51.8% |
12,752 |
|
(2) Homicide |
21.3% |
5,233 |
|
(3) Suicide |
16.3% |
4,003 |
|
(4) Cancer |
6.8% |
1,670 |
|
(5) Heart Disease |
3.9% |
961 |
Indian scenario:
The accident statistics for India are dramatic. At least 13 people die every hour in road accidents in the country, the latest report of the National Crime Records Bureau reveals13. In 2007, 1.14 lakh people in India lost their lives in road mishaps — that’s significantly higher than the 2006 road death figures in China, 89,455.
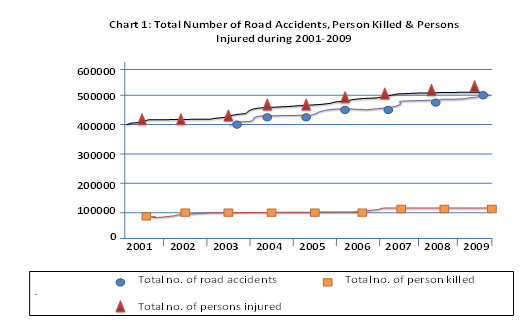
The total number of road accidents reported by all the States/ Union Territories (UTs) in the year 2009 were 4,86,384 of which 1,10,993 were fatal i.e. 22.8% of the road accidents were fatal. The number of persons killed in the accidents were 1,25,660 (i.e. an average of one fatality per 4.4 accidents). Table 2 indicates that the proportion of fatal accidents in total road accidents has consistently increased since 2001 from 17.6% to 22.8% in 2009. The severity of road accidents, measured in terms of persons killed per 100 accidents, had also increased from 19.9 in 2001 to 25.8 in 200914.
Table: 02: Number of Accidents and Number of Persons Involved: 2001 to 2009
|
YEAR |
Number of accidents |
Number of persons |
Accident severity* |
||
|
Total |
Fatal |
Killed |
Injured |
||
|
2001 |
405637 |
71219 (17.6) |
80888 |
405216 |
19.9 |
|
2002 |
407497 |
73650 (18.1) |
84674 |
408711 |
20.8 |
|
2003 |
406726 |
735809 (18.1 |
85998 |
435122 |
21.1 |
|
2004 |
429910 |
79357 (18.5) |
92618 |
464521 |
21.5 |
|
2005 |
439255 |
83491 (19.0) |
94968 |
465282 |
21.6 |
|
2006 |
460920 |
93917 (20.4) |
105749 |
496481 |
22.9 |
|
2007 |
479216 |
101161 (21.1) |
114444 |
513340 |
23.9 |
|
2008 |
484704 |
106591 (22.0) |
119860 |
523193 |
24.7 |
|
2009 (P) |
486384 |
110993 (22.8) |
125660 |
515458 |
25.8 |
|
(P): Provisional. Source: Information supplied by States/UTs (Police Departments). Figures within parentheses indicate share of fatal accidents (i.e. involving death) to total accidents. * Accident Severity : No. of Persons Killed per 100 Accidents |
|||||
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Emergency medicine – an emerging hope in India:
Quality emergency care is a fundamental individual right & should be available to all who seek it. During the French Revolution, after seeing the speed with which the carriages of the French flying artillery maneuvered across the battlefields, French military surgeon Dominique Jean Larrey applied the idea of ambulances, or "flying carriages", for rapid transport of wounded soldiers to a central place where medical care was more accessible and effective.
‘Dominique Jean Larrey’, thus, is sometimes called as the ‘father of emergency medicine’ for his strategies during the French wars.
Emergency physicians in India:
They are very few emergency physicians working in India. Most of them are concentrated in institutes which support emergency medicine's growth like Christian Medical College - Vellore, Apollo Hospitals - Hyderabad, St. John's Medical College - Bangalore, Sri Ramachandra Medical College - Chennai, etc.
Majority of the hospitals in the Apollo Group have emergency physicians looking after the administration and working of their emergency departments & emergency rooms.
Prospects of Emergency Medicine in India:
This is a difficult area to convince people about, since EM is a new in India. One thing clear is that EM will grow and develop further. We definitely expect it to grow as a specialty.
Emergency physicians can find work in any major hospitals where emergency departments exist. The only problem is that it will take a while till hospitals start phasing out casualty medical officers (CMOs) and duty doctors, and start placing emergency physicians in their place. This will happen as soon as the general public become aware and start demanding trained emergency medicine physicians to evaluate them in the emergency departments.
Emerging Opportunities in Emergency Medicine in India:
Emergency medicine by itself is an emerging opportunity in India. Apart from being consultants in EM, emergency physicians can become the best emergency department administrators, emergency medical services (EMS) directors, EMS & paramedic trainers, disaster planning consultants and first aid trainers for non medical personnel.
They can even be the best public relation officers (Due to the close association & intricate knowledge EPs have of the working of every specialty and their personnel. And due to excellent skills they have in managing any problem whether related to patients or their attenders)
Every emergency physician is trained appropriately in the latest and correct methods of cardiopulmonary, trauma and pediatric resuscitation skills. This makes them the best doctors to teach first aid and CPR skills. We are not telling that other doctors are incapable. But the nature of EM work provides ample skills needed for the EP to train anybody (whether medical or non medical) appropriately in first aid, cardiopulmonary resuscitation and trauma resuscitation.
A good emergency physician knows every single detail of the resuscitation & treatment methods of the sick & injured relating to almost every specialty. This makes the EP a great medico legal consultant who can scan medical records and point out lacunae, as well as fix them.
CONCLUSION:
Building a safer health care system means designing processes of care to ensure that patients are safe from accidental injury. Prompt recognition and efficient management of medical emergencies by a well-prepared expert team can increase the likelihood of a satisfactory outcome. The basic algorithm for managing medical emergencies is designed to ensure that the patient’s brain receives a constant supply of blood containing oxygen.
REFERENCES:
1. article.wn.com/view/2011/03/31/India_suffers_from_the_highest_number_of_road_accidents_WHO/
2. Deepak, s., S. Uday Shankar and M. Sidhyartha, 2011. A study on road traffic accidents in Anand- Gujarat. Healthline, 2: 12-15.
3. Limiya, M., 2010. A study to assess the knowledge of truck drivers regarding first aid during emergency in selected area at Bangalore, in a view of developing information booklet. Performa to Rajiv Gandhi University of Health Sciences, Karnataka.
4. Kavita, R., N. Girish and G. Gururaj, 2011. Burden, Characteristics, and Outcome of Injury among Females: Observations from Bengaluru, India. Women’s health Issues, 21: 320-326.
5. Abdou, J., J. Sundby and S. Vangen, 2011. Barriers to Emergency Obstetric Care Services in Perinatal Deaths in Rural Gambia: A Qualitative In-Depth Interview Study. ISRN Obstet Gynecol., 2011: 01-10.
6. Kanta, J., D. Kavita, 2012. Processing of management information system with in small and large scale enterprise. International Journal of Information Technology and Knowledge Management, 5: 224-226.
7. Jacobs, G., A. Aeron and A. Astrop, 2000. Estimating global road fatalities. Transport Research Laboratory, Old Wokingham road, Crowthorne, Berkshire. ISSN 0968-410.
8. Road Accidents in India, 2009. Government of India, Ministry of Road transport and Highway transport research wing, New Delhi.
9. Gururaj, G., 2002. Injuries in India: A national perspective. National Institute of Mental Health and Neuro Sciences, Bangalore, Pg. 325-347.
10. Jacob, G., A. Aeron, 2000. Road safety as a global problem. 65th road safety congress. The royal society for the prevention of accidents, Pg. 18.
11. Kareem, A., 2003. Review of global menace of road accidents with special reference to Malaysia- a social perspective. Malaysian Journal of Medical Sciences, 2: 31-39.
12. Will, H., 2000. Behavioral Factors Associated with Disease, Injury, and Death among Men: Evidence and Implications for Prevention. The Journal of Men’s Studies, 9: 81-142.
13. Laxmiprashad, 2007. Traffic management, Criminal investigation department, State crime Records Bureau, Tamilnadu, Vol. 5, Pg. 3.
14. Susan, G., B. Luke and N. Son, 2011. Are we there yet? Australian road safety targets and road traffic crash fatalities. Gargett et al. BMC Public Health, 11: 270.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






