

 About Authors:
About Authors:
Shiv Kumar Mishra, Vinita Pawar, Archana Tiwari
M.Tech Biotech
RGPV, Bhopal (MP)
Diabetes mellitus is a very common disorder in all over the world, often simply referred to as diabetes, is a group of metabolic diseases (Also known as metabolic syndrome and a slow poison) in which a person has high blood sugar, either because the body does not produce enough insulin, or because cells do not respond to the insulin that is produced. Cause classical symptoms like polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).
[adsense:336x280:8701650588]
Reference ID: PHARMATUTOR-ART-1240
SLOW POISON DIABETES SKYROCKETS
Diabetes continues to escalate worldwide. 366 million people have diabetes in world and causing DEATH OF ABOUT 4.6 MILLION PEOPLE EVERY YEAR (Approx-95% due to type-II diabetes mellitus), KILLS ONE EVERY 7 SECONDS. One in eight Indian adults either has or is at high risk of diabetes as per international diabetes federation (IDF). One in three people of America at a risk of type 2 Diabetes. 79 million diabetics in America as per American Diabetes Association (ADA). 65 million people obese by 2030 in8 America as per ADA, and obesity is the one of the major cause of diabetes. As diabetes cases are rises – health system spend $465 billion annually. Majority of diabetes caused due to- Poor diet, Obesity, lake of exercise High protein diet Raises Type 2 diabetes risk affecting- 5% global population.India leads the world with largest number of diabetic subjects earning the dubious distinction of being termed the “diabetes capital of the world”. According to the Diabetes Atlas 2006 published by the IDF, the number of people with diabetes in India currently around 40.9 million is expected to rise to 69.9 million by 2025 unless urgent preventive steps are taken. The so called “Asian Indian Phenotype” refers to certain unique clinical and biochemical abnormalities in Indians which include increased insulin resistance, greater abdominal adiposity i.e., higher waist circumference despite lower body mass index, lower adiponectin and higher high sensitive C-reactive protein levels [8].
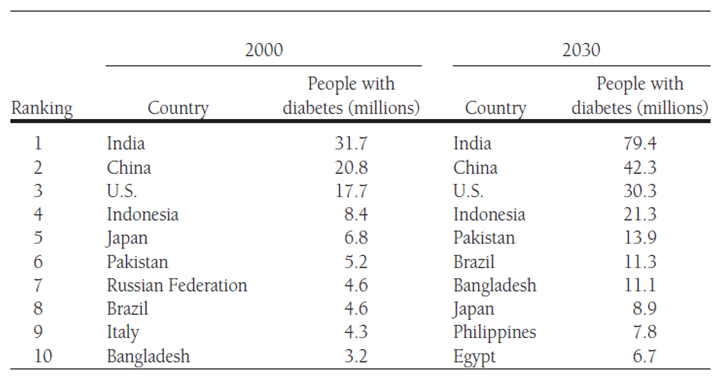
Table.1-list of countries with the highest numbers of estimated cases of diabetes for 2000 and 2030 [11]
This phenotype makes Asian Indians more prone to diabetes and premature coronary artery disease. At least a part of this is due to genetic factors. However, the primary driver of the epidemic of diabetes is the rapid epidemiological transition associated with changes in dietary patterns and decreased physical activity as evident from the higher prevalence of diabetes in the urban population [1,3,6,9]. According to the World Diabetes Atlas, India is projected to have around 51 million people with diabetes.
TYPE 1- CHILD OR JUVENILE OR (IDDM) DIABETES MELLITUS
Characterised by body's failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus (IDDM) mainly affects Childs and young individuals. Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cells of the islets of Langerhans in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune attack. There is no known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed "juvenile diabetes" because it represents a majority of the diabetes cases in children. Brittle diabetes, also known as unstable diabetes or labile diabetes refers to a type of insulin-dependent diabetes characterized by dramatic and recurrent swings in glucose levels, often occurring for no apparent reason. The result can be irregular and unpredictable hyperglycemias, frequently with ketosis, and sometimes serious hypoglycemias. Brittle diabetes occurs no more frequently than in 1% to 2% of diabetics.It is a more severe disease than type 2 diabetes, since the beta cells are destroyed by an autoimmune attack [4].
TYPE 2 DIABETES (NIDDM) OR ADULT-ONSET DIABETES OR INSULIN RESISTANCE DIABETES MELLITUS
Results from insulin resistance, a condition adult-onset diabetes in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency (Non-insulin-dependent diabetes mellitus, NIDDM). It is characterized by insulin resistance which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications that improve insulin sensitivity or reduce glucose production by the liver. Type 2 diabetes is the most common type. Indiafaces a vital health care burden due to the high Prevalence of type 2 diabetes constituting 90% of the diabetic population which preferentially affects adult individuals. Type 2 diabetes results from the interaction between a genetic predisposition and behavioural and environmental risk factors likeOverweight or obesity, abnormal cholesterol levels, cardiovascular disease risk factors (High blood pressure), History of gestational diabetes, Ethnicity and Genetics. Obesity and physical inactivity are the main nongenetic determinants of the disease [Steven et. al. M 2001]. The first national study on the prevalence of type 2 diabetes in India was done between 1972 and 1975 by the Indian Council Medical Research (ICMR, New Delhi) shows The prevalence was 2.1 per cent in urban population and 1.5 per cent in the rural population while in those above 40 yr of age, the prevalence was 5 per cent in urban and 2.8 percent in rural areas[11]. In Type 2 diabetes the body does not respond well to insulin, a hormone that helps transfer sugar out of the blood and into the body's cells and tissues, where it is used for energy.At first, the islet cells in the pancreas try to produce more insulin in an effort to make the body respond. But eventually, these cells cannot keep up and stop working altogether i.e. development of insulin resistance, so sugar stays in the blood. People with Type 2 diabetes have difficulty maintaining normal blood sugar levels.If blood sugar is not controlled, it will leads to several complications such as heart disease, stroke, hypertension, and kidney failure. Blindness and even amputation of extremities in extreme cases are also reported in patients with Type 2 diabetes due to development of blood circulation problems. An increasing number of genetic variants have been consistently found to contribute to the risk of developing Type 2 diabetes. Variants in the TCF7L2 gene appear to be associated with the highest risk of developing Type 2 diabetes, and also can predict the likelihood that a person will convert from a state of pre-diabetes (borderline blood sugar levels) to full-blown Type 2 diabetes. Several studies have shown that overweight pre-diabetics who have certain TCF7L2 variants have a 55-70% chance to develop Type 2 diabetes within 3 to 5 years after their initial diagnosis. [decodeme.com/type-2-diabetes]Type 2 diabetes is primarily characterized by insufficient insulin secretion from the pancreatic beta cells. Current therapy aims at maintaining or improving the secretary capacity of the beta cells and increasing the insulin sensitivity of the target organs. Elucidation of the mechanisms underlying insulin secretion and the malfunctions causing type 2 diabetes is expected to provide new strategies for restoring insulin secretion [5,10,12].
[adsense:468x15:2204050025]
TYPE 3- DIABETES MELLITUS
New form of diabetes discovered by Dr Suzanne de la Monte and her research team at the US Brown Medical Schooldiscovered in 2005 as a result of alzheimer’s disease research. In type 3 diabetes the brain produces lower than normal levels of brain insulin.If the brain cells are deprived of insulin they eventually die causing memory loss, Confusion and Dementia and other degenerative diseases. These diabetes type 3 symptoms mentioned above are also associated with alzheimers disease – which causes memory loss.This type of diabetes normally shows up much later in life and sometimes thought to be a normal part of aging process.
Gestational diabetes mellitus (GDM) in several aspects resembles type 2 diabetes which includes combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2%-5% of all pregnancies and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life. Apart from the lack of insulin, increased secretion of the blood glucose-elevating hormone glucagon contributes to rise of blood glucose in diabetes. An another study shows that diabetes results in a 70% reduction in rate of protein synthesis in skeletal muscles 44% reduction in that of the heart. Increases protein synthesis rate in both tissues in diabetics shown when provided with Insulin (but not in normal animals) High protein diet raises risk of Type 2 diabetes [2,7].
CONCLUSION
Diabetes is a major problem of the world. It acts as a slowpoison to an individual and moves him slowly towards death. In this situation body becomes irresponsive gradually. The above data shows that India is more prone to diabetes (with 79.4 million diabetics in 2030); India is known as the diabetic capital of the world. Above presented data also shows the prevalence of the diabetes across the world. Every country government are facing this problem and try to overcome it but till now there is no any permanent and reliable treatment of choice for diabetes. So it’s social and moral responsibility of the world community to come together to fight against such a deadly disease. Now it’s a time to act for diabetes now (to stop the effect of its slow poison), so that no one died by diabetes and make the world community free from diabetes mellitus.
References
1. Anjana, R.M., Ali, M.K., Pradeepa, R. et al. (2011). The need for obtaining accurate nationwide estimates of diabetes prevalence in India - Rationale for a national study on diabetes. Indian J Med, 133, 369-380.
2. Aggarwal, P., Gill-Randall, R., Wheatley, T. et al. (2001). Identification of mtDNA mutation in a pedigree with gestational diabetes, deafness, Wolff-Parkinson-White syndrome and placenta accreta. Hum Hered. 51, 114-116.
3. Hamid, A., ANWAR, M., Tanzeel, A. (2006). Diabetes Mellitus from Antiquity to Present Scenario and Contribution of Greco-Arab Physicians. JISHIM, 5, 46-50
4. Pugliese A. (2004). Genetics of type 1 diabetes. Endocrinolol Metab Clin N Am. 33, 1-16
5. Ramachandran, A., Snehalatha C., and Viswanathan, V. (2002). Burden of type 2 diabetes and its complications –The Indian scenario. CURRENT SCIENCE, VOL. 83,1471-1476
6. Ramachandran, A., Jali, MV., Mohan, V. et al. (1988). High prevalence of diabetes in an urban population in South India. Br Med J. 297, 587 – 590.
7. Richard, m., Watanabe., Black m.h. et al. (2007). Genetics of Gestational Diabetes Mellitus and Type 2 Diabetes. DIABETES CARE, 30 (2), S134-S140
8. Sandeep, S., Ganesan, A., and Mohan V. (2007). DEVELOPMENT AND UPDATION OF THE DIABETES ATLAS OF INDIA. Madras Diabetes Research Foundation Chennai.1-18
9. Mohan, V., Sandeep, S., Deepa, R. et al. (2007). Epidemiology of type 2 diabetes: Indian scenario. Indian J Med Res. 125, 217-230
10. Weir, G.C. and Bonner-Weir, S. (2004). Five Stages of Evolving β -Cell Dysfunction during Progression to Diabetes. Diabetes. 53(3), S16-S210.
11. Wild, S., Roglic, G., Green, A. et al. (2004). Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 27, 1047-53.
12. Wolford, Johanna, K., Vozarova de, C. Barbora, (2004). Genetic Basis of Type 2 Diabetes Mellitus: Implications for Therapy, Treatments in Endocrinology. 3 (4) 257-267
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






