

{ DOWNLOAD AS PDF }
ABOUT AUTHORS
Naga Subrahmanyeswari, Srinivasa Babu, Gajula. Supriya, Bandi . Srilekha
Vignan Pharmacy College, Vadlamudi, Andhra Pradesh
ABSTRACT:
Ebola virus disease (EVD) is previously known as Ebola hemorrhagic fever. It is a serious fatal illness to human. EVD is caused by the Ebola virus. The outbreak of Ebola virus began in the Republic of Guinea in February 2014.The 2014 West Africa outbreak is believed to be most severely recorded in medical history. Around 1440 cases with 826 deaths have been reported. But around 16,000 people survived in West Africa. A cellular protein acts as a receptor for Ebola virus and Marburg virus. TIM-1 acts as a receptor for Ebola virus which is a cellular protein. It is transmittable disease which occurs by the contact with the blood or body fluids of a person who was infected or died from EVD, contaminated objects like needles and infected animals or meat. Burial ceremonies in which mourners have direct contact with the body of the deceased person can also major role in transmission of Ebola. EVD has an incubation period of about 2 to 21 days, and the infection has an acute onset without any carrier status. At present, there is no particular type of treatment for EVD, so it is important to avoid infection exceeded 80%, modern medicine in public health measures have been taken to reduce the smack of EBD on individuals and communities. Treatment for Ebola virus involves early, truculent, supportive care with rehydration. Typical symptoms of Ebola virus disease include fever, diarrhea, nausea and vomiting for about 3-5 days and may lasts up to one week, abdominal pain. Upon increase in severity of the virus the patient may suffer from confusion, dehydration, and hypotension. These conditions eventually may lead to death. Ebola virus may be spread due to insufficient medical facilities, poor sanitation, unsafe burial practices. Ebola virus does not replicate through cell division. There is no definitive cure and management is mainly supportive ensuring adequate hydration and symptomatic treatment.
Reference Id: PHARMATUTOR-ART-2666
|
PharmaTutor (Print-ISSN: 2394 - 6679; e-ISSN: 2347 - 7881) Volume 7, Issue 05 Received On: 02/04/2019; Accepted On: 30/04/2019; Published On: 01/05/2019 How to cite this article: Subrahmanyeswari, N., Babu, S., Supriya, G. and Srilekha, B. 2019. An Overview of Ebola Virus - It’s Pathogenesis, Treatment and Vaccination. PharmaTutor. 7, 5 (May 2019), 28-33 |
INTRODUCTION:
The Ebola virus is an RNA virus belonging to family Filoviridae (Bukreyev AA et al; 2014). There are 5 different types of species namely-Bundibugyo,Sudan,Zaire,Reston and TaiForest (Diehl WE et al; 2016). Fruit bats of the Pteropodidae family are the natural Ebola virus hosts (Bukreyev AA et al; 2014).Animal to human transmission occurs by close contact with the blood, secretions, organs and other body fluids of the infected animals. Human to human transmission occurs by the direct contact with the body fluids of the infected individuals. The outbreak of Ebola virus began in the Republic of Guinea in February 2014.The 2014 West Africa outbreak is believed to be most severely recorded in medical history. Around 1440 cases with 826 deaths have been reported. But around 16,000 people survived in West Africa (Houlihan CF et al ; 2017).
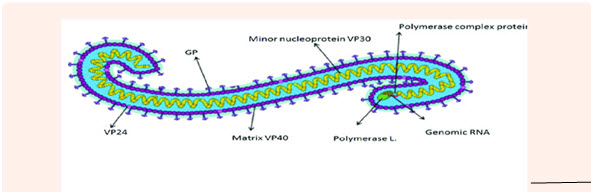
Fig.1 Structure of Ebola virus
In India:
An Indian resident have been tested positive for Ebola. He was cured and has landed in Delhi from Liberia. According to the Times the man had already been treated for Ebola in West Africa and currently doesn’t have symptoms and tested negative for the virus before he flew. But his semen tested positive for the flew. Semen can tested positive after clinical clearance for up to three months, according to Centers for Disease Control Prevention (CDC) .It not likely that he poses a threat, given the negative test from his blood; spread of Ebola in India could be ruinous in the population size.
Receptors for Ebola virus:
A cellular protein acts as a receptor for Ebola virus and Marburg virus. TIM-1 acts as a receptor for Ebola virus which is a cellular protein. It is also clear that there are other receptors for Ebola because while TIM-1 is majorly found on epithelial cells in the body, it is not found on important cell types which are infected by Ebola.
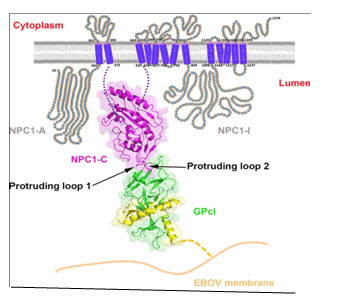
Fig.2 TIM-1 receptor
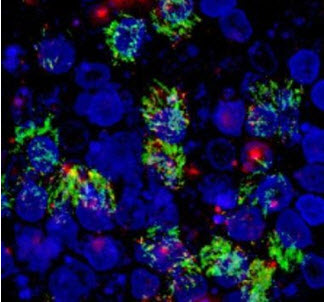
Fig.3 Microscope image shows TIM-1 expression (in green) on the surface of human airway cells.
Pathogenesis :
Virus enters the body via infected blood/body fluid in contact with a mucosal surface or a break in intact skin. Virus replicates preferentially in monocytes/macrophages and dendritic cells which facilitate dissemination of the virus throughout the body via lymphatic system. Other cells are secondarily infected and there is rapid viral growth in hepatocytes, endothelial and epithelial tissues.
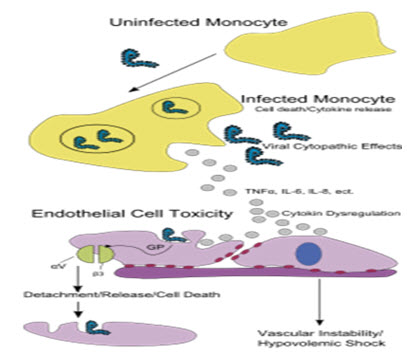
Fig-4 Pathogenesis of Ebola virus
Clinical Features:
The incubation period of Ebola was found to be 2-21 days (Ouattara E et al; 2017).
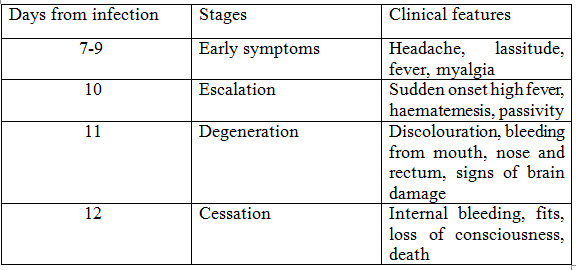
Table 1.1
Early and Late clinical features of Ebola:
Early clinical features:
• Intense tiredness, weakness, malaise
• Sudden onset of fever
• Headache
• Myalgia
• Hiccups
• Conjunctivitis (Sochas L et al; 2017)
• Nausea and loss of appetite
• Throat pain and difficulty swallowing
• Abdominal pain
• Diarrhoea
Late clinical features:
• Confusion and irritability
• Seizures
• Chest pain
• Diarrhoea(watery or bloody)
• Vomiting (sometimes bloody)
• Skin rash
• Miscarriage in pregnant women
• Shock
• Respiratory distress
Risk assessment:
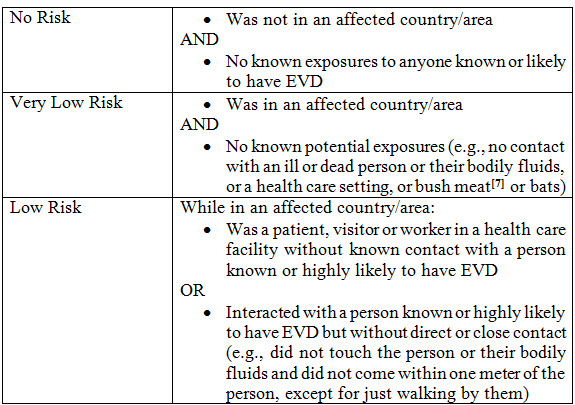
Table-1.2
Transmission:
![]()
Fig-5 Transmission of Ebola virus
Ebola can be transmitted through close contact with the blood, secretions, organs or other body fluids of infected animals. It can also be transmitted by the handling of infected chimpanzees, gorillas, fruit bats, monkeys. In community it can be spread through human-to-human transmission, which results from direct contact with blood, secretions, organs or body fluids of infected people. Burial ceremonies in which mourners have direct contact with the body of the deceased person can also major role in transmission of Ebola.
Animal to human transmission:
Animal to human transmission occurs either by direct contact with infected bats or by handling infected, dead animals including hunting, slaughtering wild animals. Care should be taken while dealing with the blood and body fluids of all animals.
Human to human transmission:
Human to human transmission occurs by the direct contact with blood, secretions, organs or body fluids of infected people. It can also be transmitted through objects (like needles and syringes) that have been contaminated with the virus.
Treatment:
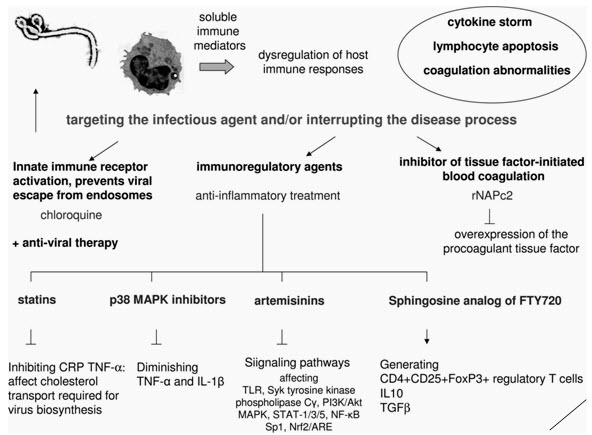
Fig-6 Treatment of Ebola virus
Oral manifestations:
Oral manifestations like Gingival bleeding, mucosal lesions, sore throat to severe dysphasia are observed. Gingival bleeding is seen along with other forms of bleeding like epistaxis and bleeding from the injection site. Dental professionals may face many patients who are not aware of the disease which are they affected. Reports show that around 1-6% of healthy individuals and 3-9% of close family members are infected without themselves developing the disease.
Ophthalmic manifestations:
COJUCTIVITIS is a key Ophthalmological EVD symptom. It is a bilateral, asymptomatic and nonicteric. In secondary EVD, conjunctivitis is the earlier symptom occurs together with influenza. It may appear 6-7 days before the patient needs EVD related care.
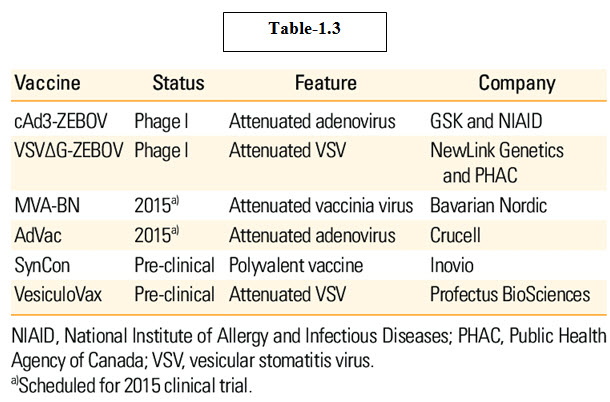
Vaccination:
CAd3-ZEBOV (also known as the NIAID/GSK Ebola vaccine or cAd3-EBO Z) is an experimental vaccine for two Ebola viruses, Ebola virus and Sudan virus, developed by scientists at GlaxoSmithKline (GSK) and tested by National Institute of Allergy and Infectious Disease (NIAID). The vaccine is derived from Chimpanzee adenovirus, chimp adenovirus type 3 (chAd3) genetically engineered express glycoprotein from the Zaire.
Conclusion:
Ebola virus disease is also known as Ebola hemorrhagic fever which is a disease of humans and other primates caused by Ebola viruses. There is no definitive cure and management is mainly supportive ensuring adequate hydration and symptomatic treatment. Prevention is done by avoiding under cooked food and bush meat, washing hands with soap and maintain proper hygiene.
REFERENCES:
1. Bukreyev AA,Chandran K ,Dolnik O et al (2014); Discussions and decisions of the 2012–2014 International Committee on Taxonomy of Viruses (ICTV) Filoviridae Study Group, January 2012–June 2013; Arch Virol; 159(4):821-30
2. Diehl WE ,Lin AE ,Grubaugh ND et al. (2016); Ebola virus glycoprotein with increased infectivity dominated the 2013–2016 epidemic; Cell. ; 167(4); 1088-1098.e6
3. Houlihan CF ,McGowan CR ,Dicks S et al. (2017); Ebola exposure, illness experience, and Ebola antibody prevalence in international responders to the west African Ebola epidemic 2014–2016: a cross-sectional study; PLoS Med. ; 14(5); e1002300
4. Ouattara E ,Duvignaud A et al. (2017); Impact of the Ebola outbreak on Trypanosoma brucei gambiense infection medical activities in coastal Guinea, 2014–2015: a retrospective analysis from the Guinean national Human African Trypanosomiasis control program.; PLoS Negl Trop Dis; 11(11): e0006060
5. Sochas L ,Channon AA ,Nam S (2017); Counting indirect crisis-related deaths in the context of a low-resilience health system: the case of maternal and neonatal health during the Ebola epidemic in Sierra Leone; Health Policy Plan; 32(suppl_3); iii32-iii39
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






